|
Arteriovenous malformations (AVMs) are congenital vascular deformities that belong to angiomas. They consist of a nidus to which the supplying arterial vessels flow in and venous blood vessels lead out. The arteries cross the nidus without the interposition of a capillary system directly into the draining veins, resulting in a high blood flow. Due to the raised blood flow and blood pressure in the draining veins they are usually gigantically extended. Furthermore, it can give rise due to the raised blood pressure to the development of aneurysms (sacculation of the vascular wall) in the arterial vessels. Due to the raised blood pressure and the aneurysm development, AVMs have a tendency to spontaneous bleeding and are as a result often symptomatic. The probability of bleeding is a subject of controversy and it depends on the kind of AVM. The bleeding risk is estimated at approximately 2% per year. In the case of bleeding in the brain or in the spinal cord severe disturbances, e.g. hemiparalysis or paraplegia, can result.
AVMs are usually noticeable due to bleeding or seizures. The symptoms of the bleeding can be very variable depending on location, and include paralyses, sensory disturbances, speech impediments, disturbances of equilibrium or vision disorders. It often leads to very severe bleeding, due to which the patient may lapse into a coma.
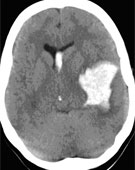
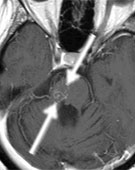
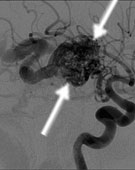
If there is a suspicion of brain bleeding, X-ray computed tomography (CT) is carried out first and the scale of the bleeding is determined (Fig. 2A). Otherwise magnetic resonance imaging (MRI) with a dose of contrast agent is carried out. This technique also permits the visualization of very small AVMs (Fig. 2B). However, the method of choice is digital subtraction angiography (DSA). Only with this technique is it possible to exactly assess the AVM architecture and the dynamics of blood flow (Fig. 2 C). Besides imaging, a neurological examination is very important. In the case of seizures also brain waves are recorded (electroencephalography).
Fig 2.
A: The CT shows severe bleeding through an AVM in the left temporal lobe.
B: The MRI shows a small AVM in the brainstem (arrows).
C: The DSA shows an AVM in the region of the basal ganglia. (arrows)
Therapy, in particular the question whether an AVM can be or has to be treated, depends on numerous factors. Theoretically treatment is necessary if the AVM was detected due to bleeding, in order to avoid further bleeding. If it is an incidental finding and the position of the AVM is awkward or the AVM is very large, it can also make sense not to carry out any treatment at all, because the risk of treatment may be higher than the risk of spontaneous progression of the disease.
If the treatment takes place, three therapeutic procedures are available: - Surgery
- Embolization
- Irradiation
The purpose of the therapy is the complete occlusion of the nidus. Partial occlusion of the nidus or occlusion of only the large supplying feeders is contraindicated, since in this way the risk of bleeding increases. Complete removal of the AVM is the therapy of choice, if it can be carried out without increased risks. By the removal of the AVM the risk of spontaneous bleeding is immediately eliminated. Often, larger AVMs are first embolized, and then surgically removed. But sometimes it is also possible for smaller AVMs to be completely embolized. In the case of small AVMs that are located in important regions (e.g. thalamus, internal capsule) precision radiation therapy (radiosurgery) can be carried out. The spontaneous bleeding risk is however – in contrast to surgery – not eliminated immediately, but only slowly decreases. Only complete removal of the AVM eliminates the risk of bleeding. Complete removal will take place only about 2 - 3 years after irradiation. Various studies have shown that approximately 80 - 90% of AVMs were cured after radiosurgical treatment (no more AVMs detectable).
If the AVM is detected due to an epileptic seizure and lies in an easily accessible brain region, indications for surgery are also present. Alternatively, epileptic medication therapy alone may be administered, as requested by the patient. If the AVM is in an area difficult to access, embolization or irradiation can be considered.
A symptomatic AVM in the spinal cord should be treated at an early stage, because there is a danger of paraplegia.
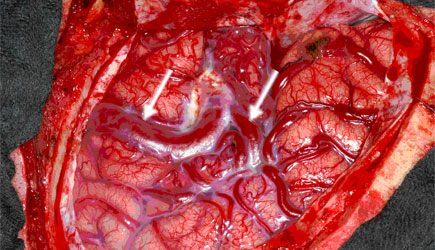
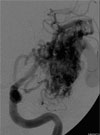
A 23-year-old student suffered initially from a generalized seizure. The MRI showed a large AVM in the left temporal lobe. The DSA showed a number of large arterial feeders that came from the middle cerebral artery. The outflow took place through a large bore superficial vein. The electroencephalography (EEG) confirmed that the cause of the seizure was the AVM. Embolization was not possible because of the high blood flow. The AVM was microsurgically completely removed through a left temporal trepanation. Postoperatively the patient has no neurological failures and is free of seizures. He continues to actively play water polo.
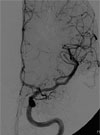
Fig. 3.
A and B: The DSA shows a large AVM with feeders from the middle cerebral artery.
C and D: The DSA after surgery shows complete removal of the AVM. The patient has been free of complaints and without neurological deficits for 6 months after surgery.
|