|
Dural arteriovenous fistulas (DAVFs) are acquired vascular deformities that can develop after an accident or spontaneously. Often they also develop after thrombosis of the venous sinus. Crucial for prognosis is venous drainage of the fistula. If drainage takes place through the cerebral veins, there is arterial blood pressure in the veins and in consequence a high risk of brain haemorrhage. In this case fistula occlusion has to take place as soon as possible. In the case of concussion it can lead to a laceration of the cerebral artery with haemorrhage in the venous cavernous sinus (carotid-cavernous fistula). Also in this case early treatment is necessary in order to prevent blindness due to high venous pressure in the eye.
DAVFs often become apparent through cerebral haemorrhage. Symptoms of the haemorrhage can be very diverse, depending on the location, and can include paralyses, sensory disturbances, speech impediments, disturbances of equilibrium and vision disorders. However, it often involves primarily severe bleeding due to which the affected persons lapse into a coma. In the case of fistulas in the ear area, a sensation of pulse synchronous bruits is typical.
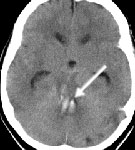
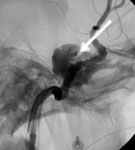
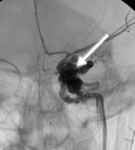
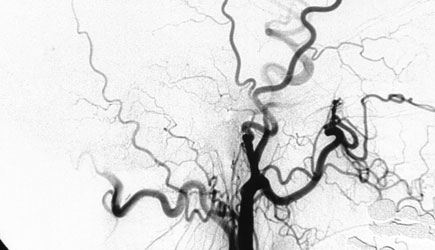
If there is a suspicion of cerebral haemorrhage, at first X-ray computed tomography (CT) is carried out. This enables the scale and location of the haemorrhage to be assessed (Fig. 1A). In order to determine the cause of the haemorrhage digital subtraction angiography (DSA) takes place, because one can precisely assess the architecture of the DAVF and the feeders only with this technique (Fig. 1 B and C). Apart from imaging a neurological examination is important.
Fig. 1. DAVF in the region of the cerebellar tentorium
A: CT of the DAVF with haemorrhage in cerebellum (arrow)
B and C: The DSA shows the DAVF (long arrows), which is fed first of all by the carotid artery. The draining vein is aneurysmally (short arrows) extended.
The aim of treatment is complete fistula occlusion. This occlusion can take place interventionally as embolization or by microsurgical surgery with fistula interruption. In the case of larger cerebral haemorrhages removal of the haemorrhage takes place at first in order to prevent a life-threatening increase of intracranial pressure. Only secondarily is the fistula then occluded. Some fistulas can be completely occluded by embolization. If this does not succeed, the remaining fistula is microsurgically occluded through an opening in the skull.
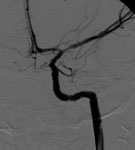
The 32-year-old female patient was injured in a road accident and suffered from severe concussion. In the course there was noticeable a rapidly progressing swelling in the region of the left eye. At first she was unconscious. Auscultation through the left eye revealed a strong bruit. The DSA carried out subsequently showed that the large carotid-cavernous fistula (carotid artery) was extensively torn and bled into the surrounding venous cavernous sinus. Because of the high arterial pressure, which was only present in the sinus, there was a danger for the left eye to become blind. With the help of a catheter introduced into the artery, the fistula was occluded by a stent (intervention carried out by senior physician Kirsch, Neuroradiology). The DSA after placing the stent shows complete fistula occlusion. After the fistula occlusion the swelling in the region of the left eye rapidly decreased in size. It was possible to save the patient’s vision.
Fig. 2.
A: Swelling in the region of the left eye.
B and C: The DSA shows the large carotid-cavernous fistula.
D and E: The DSA after placing the stent shows complete fistula occlusion.
F: Regression in the lid swelling after fistula occlusion.
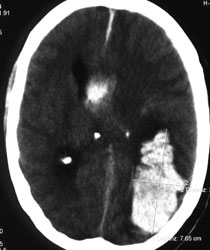
A 47-year-old man complained of acute headaches. A short time later he lost consciousness. The left pupil became white. The CT showed a large cerebral haemorrhage. The haemorrhage was removed in the course of emergency surgery. The DSA carried out subsequently showed as the cause of haemorrhage a strong DAVF with drainage by cerebral veins. The DAVF was occluded through embolization (intervention carried out by senior physician Kirsch, Neuroradiology). The post interventional DSA shows complete fistula occlusion. The patient recovered well from haemorrhage and returned to work.
Fig. 3.
A: The CT shows a large cerebral haemorrhage in the left occipital lobe.
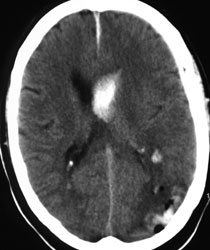
B: Postoperative CT shows removal of the haemorrhage.
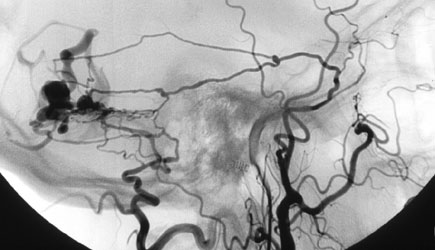
C: The DSA shows the large DAVF with inflows from the middle meningeal artery and occipital artery, and drainage by cerebral veins.
D: The DSA after embolization shows complete fistula occlusion.
E: The CT 4 months after surgery shows complete haemorrhage resorption and also the embolic agent in the region of the former fistula.
|