|
Haemodynamic cerebral ischaemia refers to insufficient blood supply of particular brain areas. The causes are usually vascular occlusions (e.g. occlusion of large carotid artery) or vascular stenoses (vascular constrictions). While a sudden occlusion of a cerebral artery often occurs together with a manifest stroke (cerebral infarction), the slowly progressive stenoses are often at first well compensated by collateral blood supply. If the stenosis exceeds a critical point, it leads however to decreased circulation in the area of supply of the particular cerebral vessel (haemodynamic insufficiency). In consequence, reversible neurological deficits primarily occur. The cause of vascular stenoses is often arteriosclerosis, metabolic disorders or excessive nicotine consumption.
Haemodynamic insufficiency manifests usually through initially reversible neurological deficits, such as paralyses, paraesthesia, numbness, speech impediments, vision disorders or failures of particular cerebral nerves. The kind of symptoms depends on the affected vascular area. While the symptoms initially often completely resolve within minutes to a few hours, permanent neurological deficits (manifest stroke) can occur with progression of the disease.
Because in the case of haemodynamic insufficiency stroke symptoms are predominant, at first as a rule X-ray computed tomography (CT) combined with computed tomography angiography (CTA) is carried out. However, often this does not reveal any pathological findings. Therefore magnetic resonance imaging (MRI) is also performed. Perfusions of the cerebral tissue can be assessed with CT as well as with MRI. This examination technique is called perfusion CT or perfusion MRI. In order to be able to accurately assess the occluded or stenosed vessels, digital subtraction angiography (DSA) is carried out during which the contrast agent is applied directly in the cerebral artery. In order to be able to measure the reserve capacity (i.e. brain adjustment ability during stronger burdens), we carry out a SPECT examination with special radioactive nuclides.
Fig. 1:
A: DSA with depiction of high-grade carotid artery stenosis (arrow). The right cerebral hemisphere is supplied with blood too little and too late.
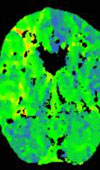
B: The perfusion CT shows a clear difference in blood supply between the right and the left cerebral hemisphere.
C: The CTA shows a well-functioning bypass (arrow)
D: The DSA shows good perfusion through the bypass of the right cerebral hemisphere (arrow).
Only a small number of strokes are based on haemodynamic insufficiency. A decisive criterion for the possibility of surgical treatment is the cerebrovascular reserve capacity. The cerebrovascular reserve capacity describes the brain adjustment ability as a reaction to increased strain. The normal cerebral tissue reacts during a respective strain with increased blood flow in the active brain area. If the cerebrovascular reserve capacity is impaired, the brain cannot physiologically react in the case of greater oxygen demand, and it leads to corresponding symptoms because of insufficient oxygen supply of the cerebral tissue. An option of surgical treatment arises only when the brain reserve capacity is depleted. In most cases, after occlusion or stenosis of the cerebral vessel, collateral circulation forms spontaneously, i.e. other vessels take over the role of blood supply by the occluded vessel. Only in the case of limited reserve capacity does the neurosurgeon have the opportunity to positively control the disease. In consequence, conducting perfusion examinations to determine the cerebrovascular reserve capacity is a decisive criterion for surgery. The second important criterion for surgery indication is the clinical symptoms. Only patients with recurrent reversible neurological deficits are candidates for surgery.
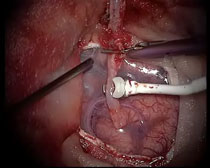
If all requirements for surgery are met, one looks for an appropriate donor vessel, depending on the location of the vascular stenosis or vascular section for revascularization. In most cases the superficial temporal artery, which is anastomosed to a branch of the middle cerebral artery, is used for bypass surgery. For this purpose the superficial temporal artery from the scalp is prepared at first, then a small opening in the skull is made, and a suitable branch of the middle cerebral artery on the brain surface is exposed. Then the branch of the middle cerebral artery is disabled and cut off from the blood supply by two clips, and the donor vessel is sewn on with a thin suture material. After completion of sutures all clips are removed and the circulation in the sewn-on vessel is checked in order to verify the patency of the anastomosis. The flow is measured with an ultrasonic probe (see video).
The video shows the microsurgical technique of the bypass surgery.
In order to start the video sequence, please click on the picture.
Already before surgery therapy with antiplatelet drugs (ASS 300 mg/day) is started. Taking this medication is continued after establishing the bypass.
A 64-year-old patient exhibited a temporary left-sided hemiparalysis. The imaging diagnostics showed an occlusion of the right cerebral artery. Fortunately, no manifest cerebral infarction was found in the computed tomography. In the perfusion measurements carried out subsequently a clearly constrained reserve capacity demonstrated itself. After administering Diamox (a vasodilating substance) it turned out that a pathological perfusion deficit (steal phenomenon) developed in the affected area of the right cerebral artery. As a result the indication was established to apply an extra-intracranial bypass (superior temporal artery on middle cerebral artery). The postoperative images clearly reveal good circulation of the right cerebral artery across the bypass. Postoperatively the patient was free of complaints. Ischaemic events did not recur.
Fig. 2.
Extra-intracranial bypass
A: The angiography of the right carotid artery shows complete occlusion of the right cerebral artery (see arrow).
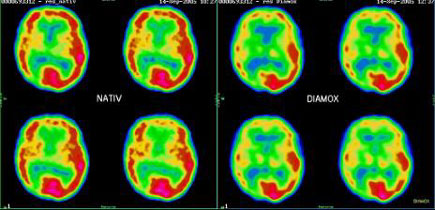
B: The blood flow examination with the SPECT technique shows insufficient perfusion of the right cerebral hemisphere (see arrow).
C: After administering Diamox (a vasodilating substance) there was a further fall in circulation of the right cerebral hemisphere, termed the ‘steal phenomenon’, which is clear evidence for an impaired reserve capacity (see arrow).
D: Preoperative angiography shows the lack of circulation of the right cerebral hemisphere in an early stage.
E: After establishing the bypass good circulation of the right cerebral hemisphere via the bypass is visible (see arrow).
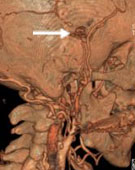
F: In the 3D reconstruction one can clearly see how the bypass from outside the skull is pulled into the skull interior (see arrow).
|