|
Cavernomas are vascular malformations composed of thin-walled blood vessels. It was previously assumed that cavernomas are congenital. Today it is known that cavernomas, like other tumours, can occur de novo. Cavernomas can occur anywhere. For the neurosurgeon the relevant cavernomas are in the brain, spinal cord or the eye socket. Cavernomas can bleed and because of that are often symptomatic. The bleeding probability is differently reported in different studies, and is approximately 1-6% per year. In the case of bleeding into the brainstem or spinal cord severe neurological disturbances can result, e.g. paraplegia.
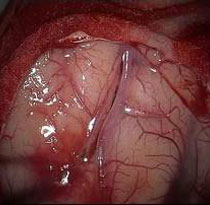
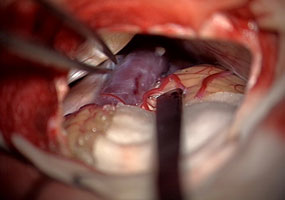
Fig. 1. Microscopic (A) and endoscopic (B) picture of a cavernoma (typically mulberry-like structure).
The symptoms can be very diverse. Many cavernomas are initially symptomatic through seizures. Depending on the location there can also occur neurological deficits, e.g. paralyses, sensory disturbances, speech impediments, disturbances of equilibrium or visual disorders. If the cavernoma bleeds more heavily, there are complaints of acute headaches.
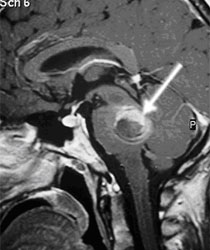
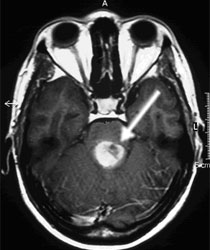
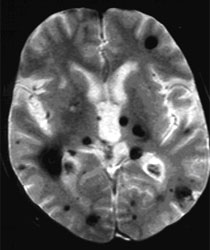
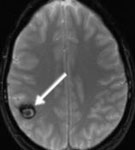
Magnetic resonance imaging (MRI) with a dose of contrast agent is the examination of choice (Fig. 2 A,D). This technique also permits the depiction of very small cavernomas. With special sequences the blood degradation products can be well recognized (Fig. 2 C). Apart from imaging neurological examinations as well as recording of brainwaves (electroencephalography) are important.
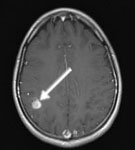
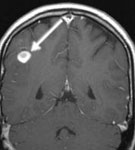
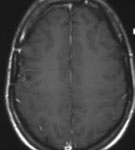
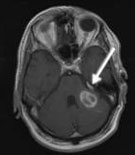
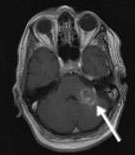
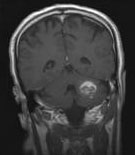
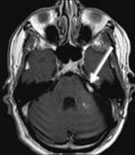
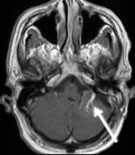
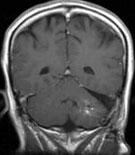
Fig. 2. Magnetic resonance imaging of cavernomas
A and B: Cavernoma in brainstem (arrows) C: multiple cavernomas D: Cavernoma in spinal cord (arrows)
Treatment, in particular the question whether a cavernoma has to be treated surgically, depends on numerous factors. Basically the complete removal of the cavernoma is the therapy of choice, if the cavernoma is or was (e.g. because of bleeding) symptomatic. If the cavernoma has bled once, there is a danger of further bleeding that is often connected with more severe neurological disturbances than the primary bleeding. Still not every cavernoma that has bled is immediately operated on. In particular in the case of brainstem cavernomas, which do not reach as far as the surface, and cause no neurological disturbances or only very small ones, it is often better to wait, because broad neurological disturbances can develop through the approach to the cavernoma alone. The position of the cavernoma is also a decisive criterion for or against surgery. In the case of progressive neurological disturbances, one has to certainly in every case immediately operate, because severe irreversible obstructions can result. Also the patient’s age is relevant. A cure is possible because of surgery. Recurrences after the complete removal of a tumour are extremely rare (so far no patient in our series). That is why complete removal of the tumour is always aimed at. In every case individual counselling of the patient is necessary.
If the cavernoma is noticed because of an epileptic seizure, and it is located in an easily approachable brain region, there is an indication for surgery. Alternatively, medication epilepsy therapy only can take place at the patient’s request. If the cavernoma is located in an area difficult to approach, it is operated on only in the case of drug-resistant epilepsy. The effectiveness of radiotherapy is so far not proved and we do not recommend it.
Symptomatic cavernomas in the spinal cord should be treated surgically at an early stage because there is a danger of paraplegia. In particular, in the case of progressing symptoms due to multi-stage cavernoma bleeding, it has to be quickly operated on.
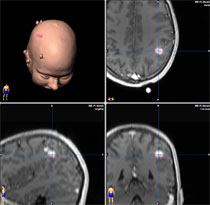
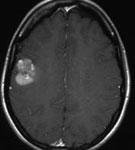
Fig. 3.
A: The MRI images show a cavernoma with haemorrhage in the postcentral region of the right cerebral hemisphere.
B: Approach planning with neuronavigation.
C: The video shows tumour removal through cerebral sulcus access.
D: Recording of brain waves by cerebral cortex.
E: Electrodes at the edge of the resection cave.
F: Postoperative T1-weighted MRI imaging with contrast agent shows complete tumour removal. The female patient remains free of complaints one year after surgery. Seizures did not occur any more after surgery (without taking medication).
The 24-year-old female patient complained of insidious hemiparalysis. The MRI showed a large precentral cavernoma. Under neuronavigational guidance the cavernoma was completely removed. The patient is postoperatively free of complaints.
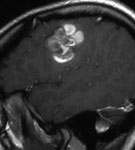
Fig. 4.
A and B: The T1-weighted MRI imaging shows a cavernoma with haemorrhage in front of the precentral region of the right cerebral hemisphere.
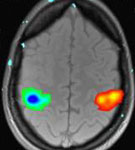
C: The functional MRI shows the localization of the motor centres for hands.
D and E: The postoperative T1-weighted MRI imaging with contrast agent shows the complete removal of the cavernoma. The patient has been free of complaints and without neurological disturbances for 3 years after the surgery.
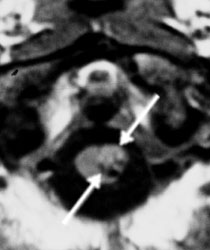
The 62-year-old patient complained of acute headaches, nausea, vomiting and disturbances of equilibrium. The MRI showed a large blood-filled cavernoma in the left cerebellar peduncle. Moreover, a large developmental venous anomaly (DVA) was associated with the cavernoma. The cavernoma was microsurgically completely removed, and the adjoining venous anomaly was left undamaged (see video). The venous anomaly has to be preserved at any cost, otherwise severe venous infarctions and congestive haemorrhage can result. The venous anomaly is a normal variant of the venous blood drainage and has nothing to do with the cavernoma, even though cavernomas are often found near venous anomalies. The patient has been free of complaints for 2 years after the surgery and no recurrence has occurred.
Fig. 5.
A: The T1-weighted MRI imaging shows a cavernoma with haemorrhage in the left cerebellar peduncle. Adjoining is a large-bore venous anomaly (arrows).
B: The video shows microsurgical removal of the cavernoma. The cavernoma is carefully dissected from the thin-walled vein and completely removed without damaging the venous anomaly.
C: The postoperative T1-weighted MRI imaging with contrast agent shows the complete cavernoma removal and the intact venous anomaly (arrows). The patient has been free of complaints and without neurological disturbances for 2 years since the surgery.
|