|
Acoustic neuroma is a benign tumour originating from the Schwann cells of the nerve responsible for equilibrium (vestibular schwannoma is thus a more correct term). Since the aforementioned nerve (vestibular nerve) runs together with the nerve responsible for hearing (cochlear nerve) and motor function of the face (facial nerve) in a bony canal, tumours compressing increasingly all three nerves cause characteristic clinical symptoms.
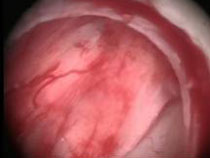
Fig. 1: Microscopic (A) end endoscopic (B) image of acoustic neuroma
Hearing impairment is the most common symptom, with time worsening to deafness. Some patients initially experience vertigo. Paralysis of the face manifests itself at later stages, in cases of larger tumours. Very large tumours may sometimes lead to abnormal accumulation of cerebrospinal fluid, with hydrocephalus as a consequence. Typical symptoms of the latter conditions include nausea, vomiting and later altered consciousness.
Magnetic resonance imaging (MRI) with contrast agent is the diagnostic procedure of choice. It allows one to find even very small tumours. Using CISS sequence (constructive interference in steady-state) single cerebral nerves inside the auditory canal and the exact extent of the tumour can be revealed (Fig. 2). Apart from imaging, clinical examination by a laryngologist is very important to assess hearing loss and disturbed sense of balance.
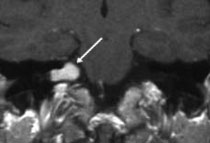
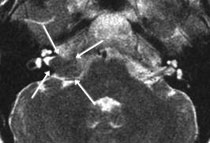
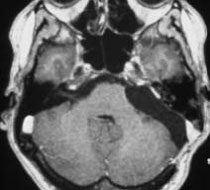
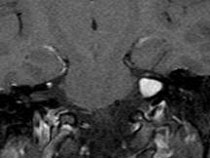
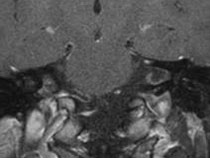
Fig. 2: MRI scan of acoustic neuroma
A: T1-weighted scan showing contrast-enhanced tumour in the cerebellopontine angle (arrow).
B: CISS sequence clearly showing the extent of the tumour in the inner auditory canal (arrows).
There are three main alternatives:
1. Regular follow-up examinations using MRI imaging
2. Microsurgical tumour removal
3. Radiotherapy
In senior patients with small tumours, basically without clinical symptoms, regular check-ups at 6-month or 1-year intervals pose a viable option. We know numerous patients with small tumours not showing any tendency to grow. Younger patients are more often qualified for surgical treatment. Especially in the case of small tumours, in patients with no significant hearing loss, there is a good chance of a good outcome. In patients with larger tumours (> 3 cm) complete hearing preservation is almost never possible. In patients suffering from serious concomitant diseases, with high anaesthesia risk, radiotherapy can be performed. Since acoustic neuroma is pathologically a benign tumour we advise mostly microscopic surgical tumour removal with endoscopic control, under monitoring of facial nerve and acoustic nerve functions. Functional monitoring enables preservation of motor function of the facial nerve even in the case of larger tumours (Fig. 3). The endoscope allows detailed inspection of the inner auditory canal and removal of remaining fragments of the tumour that could not be identified under the microscope.
Smaller tumours can be treated using radiotherapy. In patients with larger tumours we generally advise surgical treatment, since numerous cases of tumour recurrence after radiotherapy as a single method are known to us. Surgery in cases of tumour recurring after radiotherapy is more difficult, with higher risk of facial paralysis which follows from infiltration of the adjoining structures.
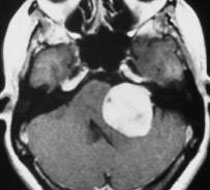
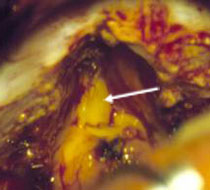
Fig. 3. A: MRI scan showing a large acoustic neuroma on the left side. B: View through an operating microscope. Tumour in cerebellopontine angle is revealed through a small craniotomy (2 x 3 cm). The inner auditory canal had to be opened, since the tumour reached there. Using both microscopic and endoscopic techniques the tumour could be completely removed. The hearing could be preserved.
A 33-year-old patient complained about hearing impairment on the left side. The MRI showed a small, mainly intrameatal acoustic neuroma. The tumor was revealed in the cerebellopontine angle via a small, approx. 2 x 3 cm craniotomy. Since the tumor reached the internal auditory canal, it had to be cut open. Under microscopic and endoscopic visual control the tumor was completely removed. Hearing was maintained.
Fig. 4
A:T1-weighted MRI scan using contrast agent showing mostly intrameatal acoustic neuroma on the left side.
B: Tumour operation using microscopic view.
C: Removal of the tumour under the microscope. Distal pole of the tumour is not visible.
D: Using an endoscope the distal part of the tumour could be removed (30° angle).
E: Final inspection using 70° angle reveals complete removal of the tumour with facial and acoustic nerves intact.
F: Post surgical T1-weighted MRI scan with contrast agent on the 7th day after the surgery showing complete removal of the tumour.
Click to start the video.
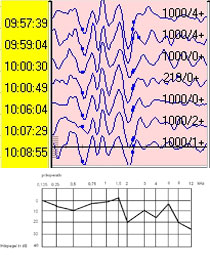
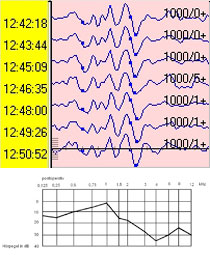
Monitoring unit for auditory and motor functions (facial nerve)
The following curves show the function of the acoustic nerves before and after removal of the tumour. Hearing function could be preserved at a significant level.
|