|
Intraventricular tumours are fully or partly located in cerebral ventricles and often lead to retention of cerebrospinal fluid through relocation of cerebrospinal fluid pathways. Because of the expansion of ventricles they are later ideal for endoscopic access.
In relation to histology the spectrum comprises basically all kinds of tumours (giant cell astrocytomas, pineal tumours, ependymomas, germinomas, primitive neuroectodermal tumours, plexus papillomas, craniopharyngiomas, pituitary adenomas, cavernomas, lymphomas).
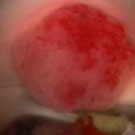
Fig. 1. Endoscopic image of ependymoma (A) and lymphoma (B). Microscopic image of plexus papilloma (C).
The majority of intraventricular tumours are noticed due to relocation of cerebrospinal fluid pathways with secondary hydrocephalus. It results in headaches, nausea, vomiting and in the chronic course also gait abnormalities, mental prostration and urinary incontinence.
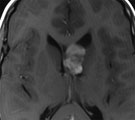
Magnetic resonance imaging (MRI) with a dose of contrast agent is the examination of choice. The MRI examination takes place at three levels: assessment of tumour location and extent, assessment of disturbance of fluid passage (hydrocephalus), and also simultaneously access planning for the surgical intervention.
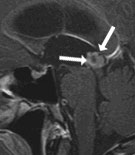
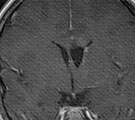
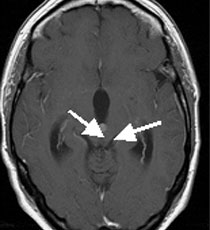
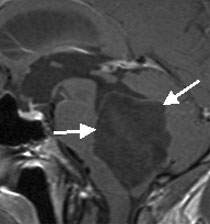
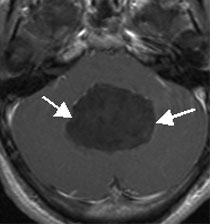
Fig. 2.
A: Magnetic resonance imaging (MRI) of a tumour in the third ventricle (pineocytoma) (arrows).
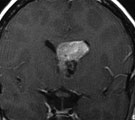
B: Tumour in the right lateral ventricle (neurocytoma) (arrows).
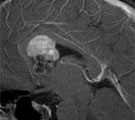
C: Tumour in the fourth ventricle (haemangioblastoma) (arrows).
In most intraventricular tumours complete removal is the therapy of choice. Since the majority of these tumours are benign, no further actions have to be taken. By removing the tumour the cerebrospinal fluid circulation is usually restored. In malignant tumours radiotherapy and/or chemotherapy takes place after the surgery. Whether a microsurgical or endoscopic surgical technique is applied depends on the size and kind of tumour, tumour location and width of ventricles. In the case of some tumours only the retention of cerebrospinal fluid is at first endoscopically treated and a sample from the tumour is taken. After having histological diagnosis further therapy (surgery, radiotherapy or chemotherapy) is decided on.
An 8-year-old girl presented with seizures and headaches. The MRI examination showed a tumour in the left lateral ventricle. Since the ventricles were very narrow, the tumour was microsurgically completely removed under neuronavigation control. It was a giant cell astrocytoma. The patient has been after surgery without neurological deficits. The headaches resolved.
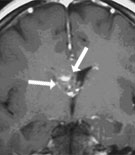
Fig. 3.
A: The MRI shows the contrast enhancing tumour in the left lateral ventricle.
B: After division of the corpus callosum one can recognize the grey-red tumour (arrows).
C: The MRI 1 year after surgery shows complete tumour removal.
The 49-year-old patient was admitted due to headaches, nausea, vomiting and disturbances in equilibrium. The MRI examination showed a tumour in the posterior part of the third ventricle with relocation of the aqueduct (connection between the third and fourth ventricle) and retention of cerebrospinal fluid (hydrocephalus). Since the ventricles were very wide and the tumour was small, purely endoscopic surgery was carried out. The video shows the entire endoscopic removal of the tumour (ependymoma) via an 8 mm large borehole. By the surgery the tumour was removed and the disturbance of cerebrospinal fluid circulation was eliminated. Postoperatively the described symptoms resolved completely.
Click to start the video.
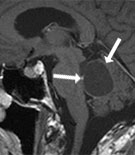
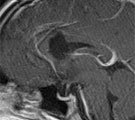
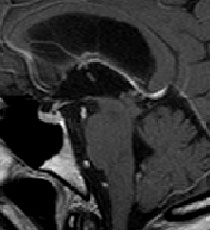
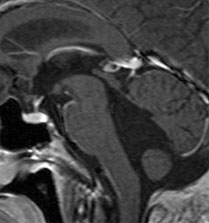
Fig. 4.
A: The MRI shows the contrast enhancing tumour in the posterior third ventricle just before the entry to the aqueduct. The ventricles are clearly expanded.
B: The video shows the complete endoscopic tumour removal. The histological examination showed ependymoma.
C: The MRI 5 years after the surgery shows complete tumour removal without recurrent tumour. The aqueduct is widely opened (arrow).
The 27-year-old patient was admitted due to nausea, vomiting and disturbances of equilibrium. The MRI examination showed a gigantic tumour in the fourth ventricle. Since the fourth ventricle was completely filled by the tumour, microscopic surgery was carried out. The video shows the complete removal of the tumour (epidermoid). Six months after surgery the patient remains free of complaints. Neurological findings are not noted.
Click to start the Video.
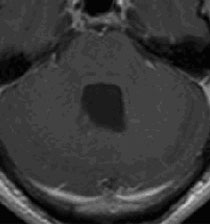
Fig. 5.
A: The MRI shows a large, non-contrast enhancing tumour in the fourth ventricle. The fourth ventricle is clearly expanded.
B: The video shows the complete microscopic tumour removal. The histological examination revealed an epidermoid.
C: The MRI 6 months after surgery shows complete tumour removal.
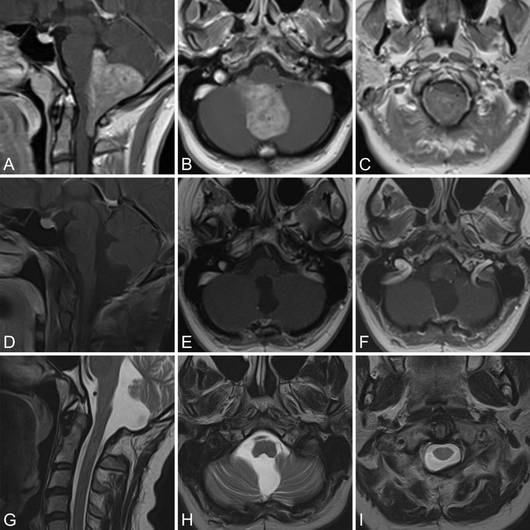
The 29-year-old woman had complained about headache and cervicobrachialgia on the right side for 1 year. MRI showed a giant contrast-enhancing mass in the fourth ventricle extending down to the level of C2 (Figure 6A–C). The clinical examination was unremarkable. No hydrocephalus was present.
The patient underwent GTR under neuromonitoring using the 4-hand suction-irrigation technique. Postoperatively, a slight apraxia of the right hand was noted for some weeks. No permanent neurologic deficits occurred. The postoperative MRI (Figure 6D-F) and the MRI from the last follow-up 14 months after surgery showed no tumor residual (Figure 6G–I).
The 32-year-old woman had complained about headache, dizziness, and intermittent anisocoria. MRI showed a contrast-enhancing mass in the fourth ventricle and consecutive hydrocephalus (Figure 7A–C). The clinical examination was unremarkable.
The patient underwent GTR under neuromonitoring using the 4-hand suction-irrigation technique. Postoperatively, a right-sided VI nerve palsy was present for some days. Furthermore, a right-sided palsy of the IX and XII nerves was present for about 2 weeks. All deficits resolved completely. The postoperative MRI showed no tumor remnants, but progressive ventriculomegaly and the patient suffered from progressive headache. Therefore, on the second day after surgery, an endoscopic third ventriculostomy was performed. The postoperative course was uneventful. The postoperative MRI and the MRI from the last follow-up 32 months after surgery showed no tumor residual and no hydrocephalus (Figure 7D–F).
|