|
Meningiomas are tumours that come from meninges and are usually (> 95%) benign. They constitute approx. 20-30% of all brain tumours and are therefore fairly common. They usually grow very slowly and initially suppress the cerebral tissue without damaging it. Because of that they can achieve considerable sizes before they are clinically noticeable. The tumours occur most often in the 5th to 7th decade of life and are more common in women than men (ratio 2.5 : 1).
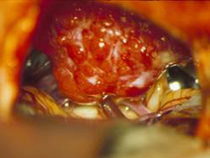
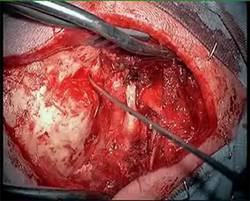
Fig. 1. Microscopic (A) and endoscopic (B) image of meningioma
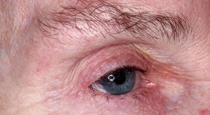
The symptoms can be very varied. They are determined by the tumour size (symptoms of cerebral pressure in the case of large tumours) and the tumour location (e.g. hemiparalysis in the case of tumour in the central motor region (Fig. 2)), and cranial nerve disorders in skull base tumours (Fig. 3C). However, even very small tumours can induce symptoms due to their unfavourable position (Fig. 3A). Meningiomas can also lead to a blockage of cerebrospinal fluid pathways resulting in the retention of cerebrospinal fluid and the development of hydrocephalus. The typical symptoms are then headaches, nausea, vomiting or in chronic development mental deterioration and gait disorder. Large tumours in the frontal lobe region usually cause slow progression of character changes that are perceived neither by the patients nor by their relatives due to slow development.
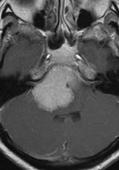
Magnetic resonance imaging (MRI) with application of a contrast agent is the examination of choice. This technique permits the visualisation of even very small tumours (Fig. 2A). Apart from the imaging, a neurological examination as well as – depending on the tumour location – an ENT and ophthalmological interview to examine hearing, equilibrium and vision abilities are important.
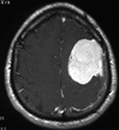
Fig. 2 Magnetic resonance imaging of meningioma in the precentral region that caused a hemiparalysis.
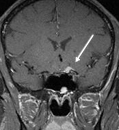
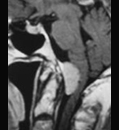
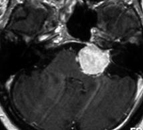
Fig. 3 A: Small meningioma (arrow) growing in the left optic canal that led to blindness. B: Meningioma in the foramen magnum with compression of the brainstem that caused a paralysis from arms to legs. C: Meningioma in the cerebellopontine angle that led to tinnitus and hearing impairment.
The therapy of choice is complete tumour removal. A cure is possible due to surgery. Recurrences are rare (in our series approx. 5%) after complete tumour removal. However, complete tumour removal is not attempted at any cost. If the tumour infiltrates functionally important structures and complete tumour removal would lead for certain to severe neurological deficits (e.g. paralysis, double images), a small tumour remnant is left and afterwards monitored with regular MRI imaging. In the case of tumour growth, precision radiotherapy (e.g. radiosurgery) is carried out. Not all meningiomas have to be obligatorily and immediately removed. In the case of small tumours that are discovered accidentally and do not cause any symptoms one can wait and monitor the condition (in particular in older patients). Primary radiotherapy is carried out only in the case of small tumours and operating contraindications (e.g. high risk of anaesthesia due to heart or lung disease) or the particular wish of the patient.
In operations on skull base meningiomas the endoscopic-assisted microsurgical technique has been established. Because of the use of the endoscope one can see round nerves and vessels as well as bony corners of the skull base. Due to that the extent of the surgical procedure is reduced. Extended skull base accesses, in which large parts of the skull base are removed, can be avoided. Often it is also possible to succeed in removing larger tumours via small and sparing openings in the skull (keyhole surgery) (Fig. 4). Generally, by applying endoscopically-assisted techniques a less invasive surgery results.
The 61-year-old female patient complained of progressive vision deterioration. The ophthalmological examination showed almost complete left blindness and severe restriction of the field of right vision. The MRI showed a large meningioma of the frontobasal region with relocation and compression of the visual nerves. Via an eyebrow incision and a small, approx. 2 x 2.5 cm craniotomy the tumour was completely removed under microscopic and endoscopic visual control. In the course of this the tumour had to be sharply dissected from the anterior cerebral artery. It was seen with the endoscope into the optic canal and the tumour was removed there under endoscopic visual control. The acuteness of vision had improved on the right with further existing hemianopsia. On the left side no improvement according to expectations appeared since the optic nerve was already seriously damaged (paper thin remaining nerve). The cosmetic result of the eyebrow incision is excellent, with a hardly visible scar.
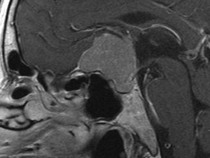
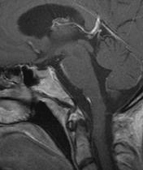
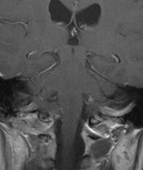
Fig. 4.
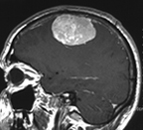
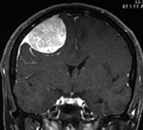
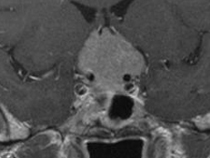
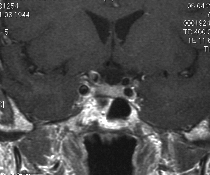
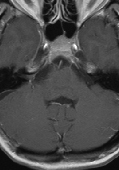
A and B: T1 weighted sagittal and coronary MRI images with contrast agent show a large tuberculum sellae meningioma with chiasma compression.
C: Access via eyebrow incision.
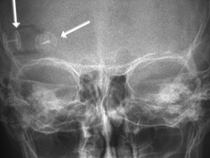
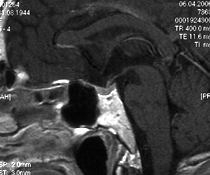
D: The postoperative skull imaging shows a small supraorbital craniotomy (arrows). E and F: The postoperative T1 weighted MRI images with contrast agent show complete tumour removal. G and H: Good cosmetic result with hardly visible scar 6 months after surgery.
The 46-year-old female patient complained of headaches. The MRI showed a large petroclival foraminal meningioma with relocation and compression of the brainstem. Due to the brainstem compression a potentially life-threatening situation occurred. Tumours in this region are among the most challenging tumours in neurosurgery because they overgrow numerous important cerebral nerves and blood vessels and because of that the surgery is technically very difficult. Still it was possible to remove the tumour completely via a wide side access under microscopic and endoscopic visual control. The patient has recovered very well from the long operation. There is only a deficiency of tongue musculature and hoarseness.
Video 2 (3.1 MB)
Click to start the video.
Fig. 5.
A: T1 weighted MRT images with contrast agent show a large meningioma with brainstem compression.
B: Postoperative T1 weighted MRT images with contrast agent 1 year after surgery show complete tumour removal. The brainstem is exposed.
C and D: The patient 6 months after the surgery. Good result without facial paralysis, eye muscle paralysis or limb paralysis.
|