|
Pituitary tumours are almost always benign tumours that originate from the cells of the pituitary gland. Pituitary tumours grow slowly and become evident either through an endocrine disorder or through compression of adjoining nerves. They often cause a typical constraint of vision due to pressure on the optic chiasma. This is manifested through a typical tunnel vision or decreasing acuteness of vision. It occasionally leads to a sudden visual disorder connected with strong headaches due to a haemorrhage in the tumour (pituitary apoplexy).
Hormone-producing pituitary tumours manifest typical endocrinological disturbances (see acromegaly, Cushing’s syndrome, prolactinoma). Due to the corresponding clinical symptoms these tumours are often discovered even though the tumours themselves are very small.
Non-hormone-producing pituitary tumours can also manifest a lack of hormones (hypopituitarism). Due to the growth of the tumour the normal pituitary gland is compressed and the individual hormone axes can then be impaired to a varying extent. Typical symptoms are a decrease in performance, exhaustion, increased need for sleep, impotence and loss of libido. Unrecognized and untreated conditions of hormone deficiency can lead to coma or death.
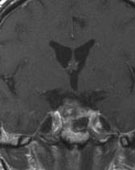
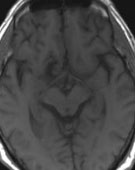
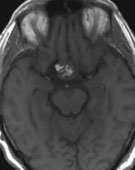
Magnetic resonance imaging (MRI) is the examination of choice in order to display pituitary tumours. Pituitary tumours are usually solid and absorb the contrast agent. However, they can also be cystic (Fig. 1). Very important for the treatment is the hormonal diagnostics in order to determine the hormones and their regulation. These examinations are carried out in the Department for Endocrinology (head: Priv.-Doz. Wallaschofski) of the Clinic of Internal Medicine A. Also after the surgery each patient has to undergo endocrinological tests in order to analyse the functional state of the pituitary gland. This is vital because some conditions of hormone deficiency can be life threatening. Finally all patients are presented to the ophthalmologist in order to objectify visual disorders.
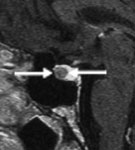
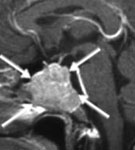
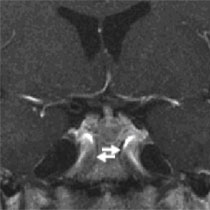
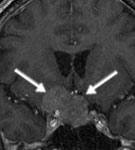
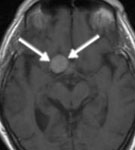
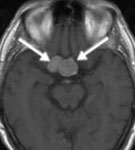
Fig. 1.
A: Intrasellar microadenoma (arrows).
B: Large cystic macroadenoma with visual nerve compression (arrows).
C: Invasive-infiltrating growing macroadenoma with destruction of the bony skull base (arrows).
In the majority of pituitary tumours the therapy of choice is surgery. Most pituitary tumours are operated on via access through the nose. In a few tumours additional surgery from above with opening of the skull and access under the frontal lobe is necessary. If the complete tumour removal succeeds, a cure is possible. However, recurrences can occur even after complete removal, since some tumours grow invasively and infiltrate the adjoining bone or venous cavernous sinus. Only if surgery is not possible, recurrences occur or the hormonal overproduction due to hormone active tumours cannot be sufficiently decreased by surgery is radiotherapy and/or medication therapy necessary. But in the case of prolactinomas an attempt at medication therapy is made primarily. Surgery is indicated if the tumours do not respond to medication therapy or alternatively the side effects of the medication therapy are so strong that it has to be discontinued.
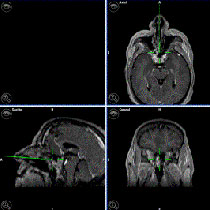
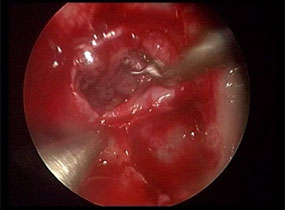
At first the right or the left nasal meatus is widened and the pituitary speculum inserted. Then the front wall of the sphenoidal sinus is opened. Through the sphenoidal sinus one reaches directly to the bottom of the pituitary fossa. The latter is opened with a drill or a swage. After the incision of the dura mater in the region of the bottom of the pituitary fossa one comes usually immediately upon the tumour, which is typically whitish and deliquescent. The tumour can usually be readily separated from the yellowish normal pituitary tissue. The tumour is then removed with various curettes and tenaculum forceps. With the assistance of the endoscope it can be seen round the bony edges during the surgery, whereby the extent of the skull base opening is minimized and the surgery trauma is reduced. By the use of the endoscope with various visual angles (30°, 45° and 70°) also the tumour parts can be recognized that are in particular niches which cannot be seen with the microscope in a straight line (see Fig. 3 with video). Due to that the radicality of the surgery can be increased. Since one can see better with the endoscope also the normal structures (cerebral artery, visual nerve as well as pituitary stalk), also the risk of surgery is minimized. Even in very large pituitary tumours one usually succeeds to identify and to protect the normal remaining pituitary gland. Intraoperative X-ray imaging (image converter) is not necessary since one can endoscopically orientate very well in the nose. In the case of repeat operations or inconvenient anatomical conditions we apply intraoperative neuronavigation, in order to be able to plan the surgical access accurately to the millimetre. Because of this the surgery risks, such as injury of the cerebral artery, are considerably reduced (Fig. 4). After the tumour is completely removed, depending on the tumour size, the adipose tissue seal that is taken from the navel region is applied. This serves to prevent the formation of a cerebrospinal fluid fistula. The surgical technique used by us does not require blocking of the nostrils with tamponades so the nasal breathing remains free. The postoperative complications are minimized due to the minimally invasive surgical technique, so the patients have hardly any complaints already on the first day after the surgery (Fig. 5).
Most pituitary tumours are operated on mainly through the nose. We prefer the endoscope-assisted microsurgical technique with endonasal access. Fig. 2A shows the setup in the operating theatre with the microscope and the endoscope. The endoscope is fixed at a pneumatic supporting arm. Opposite to the surgeon there is a video motor on which the surgery can be followed. In Fig. 2B one can see a close-up with the nasal speculum in the right nostril and the inserted endoscope. In Fig. 2C the bimanual operation is shown next to the fixed endoscope. By access directly through the nostril (endonasal access) separation of the mucous membrane from the nasal septum is avoided. That is why no tamponade displacing the nasal breathing has to be inserted in the nose after the surgery.
The video shows the endoscopic-assisted microsurgical surgery of a large pituitary tumour that spread above and adjacent to the pituitary gland region. The surgery took place by the right nostril. Under the visual control of the 70° perspective the tumour part above and next to the pituitary gland region could be completely removed. This part of the tumour was not visible with the operating microscope. This example shows well how the endoscopic technique can increase the radicality of the surgery. After the tumour removal the adipose tissue seal was applied, in order to prevent a cerebrospinal fistula. The postoperative MRI shows complete tumour removal and the inserted adipose tissue seal.
Fig. 4.
A: The preoperative MRI shows the large pituitary tumour (arrows) that spread upwards and right next to the pituitary gland region (supra- and parasellar)
B: The video presents the removal of the tumour under microscopic and endoscopic visual control.
C: The postoperative MRI confirms complete tumour removal and shows the applied adipose tissue seal.
|