|
In Cushing’s syndrome excessive ACTH (the hormone that controls the release of the adrenal hormone cortisol) is produced by a pituitary tumour. Similar to acromegaly, also in Cushing’s syndrome typical external visible changes appear. For Cushing’s syndrome full moon face, central obesity, reddish stretch marks (striae rubrae), general muscular atrophy, increased blood sugar levels, osteoporosis as well as increased arterial blood pressure are typical. If not treated, life expectancy may be considerably shortened.
The typical symptoms are central obesity, full moon face, reddish-bluish stretch marks as well as a clear muscular atrophy (Fig. 1). Patients are often diagnosed due to signs of diabetes mellitus as well as increased arterial blood pressure.
Fig. 1. Typical stigmata of Cushing’s syndrome.
A: Central obesity
B: Full moon face
C: Striae rubrae
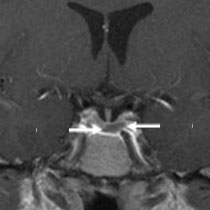
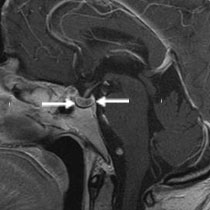
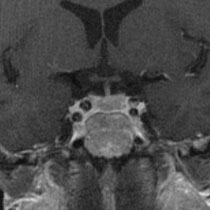
In the magnetic resonance imaging (MRI) one can often recognize very small, compared to the normal pituitary gland, less contrast enhancing roundish structures. However, occasionally the MRI shows no tumour at all, so it is very difficult to locate the hormone producing tumour. In order to be able to determine the position in which the hormone production originates, a blood sample is usually taken from the inferior petrosal sinus to be able to determine the gradient of the hormone levels in lateral comparison. Other excessive cortisol releasing processes have to be differentiated from Cushing’s syndrome. Detailed endocrinological diagnostics is important in order to test the performance of all pituitary gland axes.
Fig. 2. MRI of a patient with Cushing’s syndrome. A small, low contrast enhancing tumour (arrows) is visible at the bottom of the hypophyseal fossa.
The therapy of choice is microsurgical tumour removal. Here we choose endonasal access within the microsurgical endoscope-assisted technique. The tumour is often not easy to detect. The normal pituitary gland tissue has to be resected first. Then one comes upon a whitish deliquescent tumour, which is completely removed. However, occasionally no circumscribed adenoma is found but a diffuse mamillary adenoma of the pituitary gland. Then the pituitary gland has to be inspected inch by inch and the corresponding tumour tissue has to be removed. If the Cushing’s syndrome cannot be cured by surgery, radiotherapy or complete hypophysectomy is carried out. Sometimes also the adrenal glands have to be removed to inhibit the excessive cortisol production.
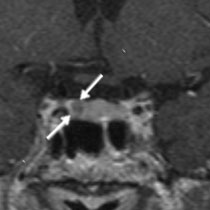
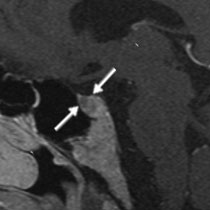
The 34-year-old man presented with typical changes in Cushing’s syndrome such as full moon face, central obesity, reddish stretch marks in the abdominal region, increased blood sugar level and high blood pressure. The endocrinological diagnostics manifested pathologically increased levels of ACTH (hormone that controls the release of adrenocorticosteroids) and cortisol. The MRI shows a small, low contrast enhancing process within the pituitary gland that might correspond to the ACTH producing adenoma. As a result an indication for surgery is established. The tumour was completely removed with the assistance of an operating microscope and endoscope. The levels of ACTH and cortisol have in consequence become normalized. The postoperative MRI shows complete removal of the adenoma. One year after the surgery the signs of Cushing’s syndrome have already resolved well.
Fig. 3. Cushing’s syndrome
A: Full moon face.
B: Preoperative MRI with image of microadenoma (arrows) that is visible on the right side at the edge of the bony skull base.
C: Postoperative MRI 1 year after the surgery shows complete removal of the pituitary adenoma. The normal pituitary gland is visible on the right side.
D: One year after the surgery the typical changes in Cushing’s syndrome have already resolved well. The normal pituitary gland functions properly, so replacement of pituitary hormones is not necessary.
|