|
Pineal cysts are benign cystic structures that originate in the pineal gland. If they exceed a certain size, they narrow the aqueduct (connection between the third and fourth ventricle) and lead to retention of cerebrospinal fluid with development of hydrocephalus. Sometimes it is difficult to differentiate pineal cysts from pineal tumours.
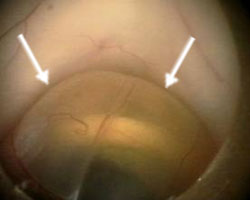
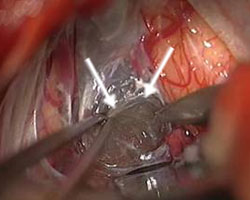
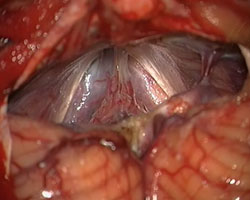
Fig. 1.
A: Endoscopic image of a pineal cyst (arrows).
B: Microscopic image of a pineal cyst (arrows).
Pineal cysts manifest in childhood or early adulthood through clinical symptoms such as headaches, nausea, vomiting, visual disorders or disturbances of equilibrium. Often intermittent symptoms occur that are probably caused by a valve effect of the cyst. However, pineal cysts are often incidental findings not responsible for the symptoms that led to the imaging.
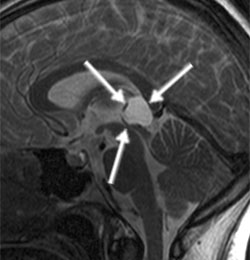
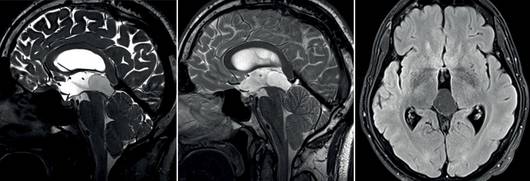
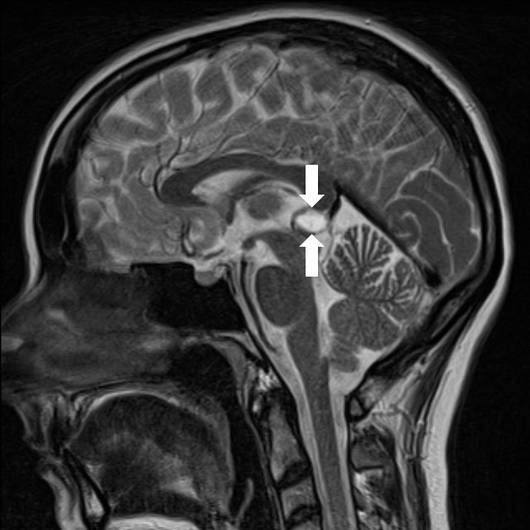
Magnetic resonance imaging (MRI) is the imaging of choice since one can exactly assess the cyst as well as the aqueduct. In particular, the sagittal sequences are important for the presentation of a possible aqueduct compression.
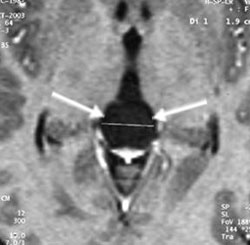
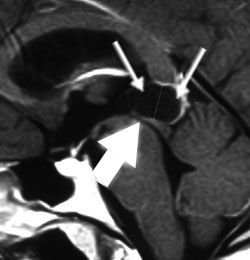
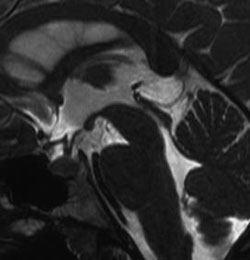
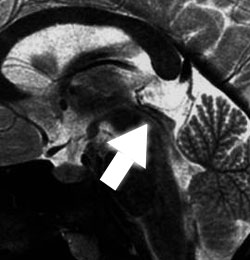
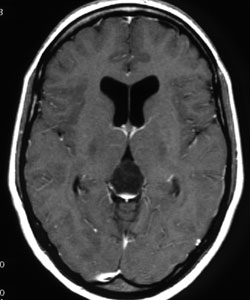
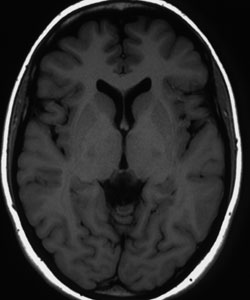
Fig. 2 MRI of a pineal cyst in sagittal and axial sectional plane. One can see the displacement of the aqueduct (thick arrow) by the cyst (thin arrows).
Asymptomatic pineal cysts that are small and cause no disturbances of cerebrospinal fluid circulation should be monitored at wider intervals (at first approx. annually) by cerebral imaging (MRI) in relation to the size and aqueduct compression. Symptomatic cysts that cause disturbances of cerebrospinal fluid circulation should be operated on.
Basically there are two surgical methods available. In the case of the extended ventricle system we prefer the endoscopic technique, in the case of narrow ventricles the microsurgical technique. Using the endoscopic technique, the surgery is carried out via a borehole at the forehead-hair border. After inserting the endoscope into the third ventricle, the pineal cyst is opened under endoscopic visual control with special instruments (endoscopic scissors, tenaculum forceps, coagulation electrodes and suction catheter) and widely fenestrated. Complete removal is usually not carried out (see video 1).
In the case of narrow ventricles the cyst is microsurgically completely removed in a sitting position via access between the cerebellar and the cerebellar tentorium. Different methods have their own advantages and have to be individually applied considering the anatomical conditions.
The MRI follow-up takes place after the surgery. In the case of complete cyst removal no further follow-ups are necessary. In the case of partial resection long-term follow-ups with regular MRI imaging take place since recurrences are possible.
The 20-year-old female patient complained of intermittent headaches, nausea and vomiting. The MRI showed a large pineal cyst that narrowed the aqueduct and already caused considerable ventricle extension. The cyst could be widely fenestrated endoscopically. The symptoms resolved completely.
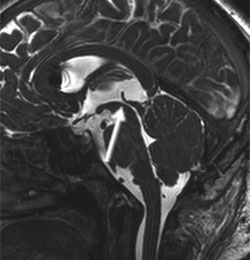
Fig. 3
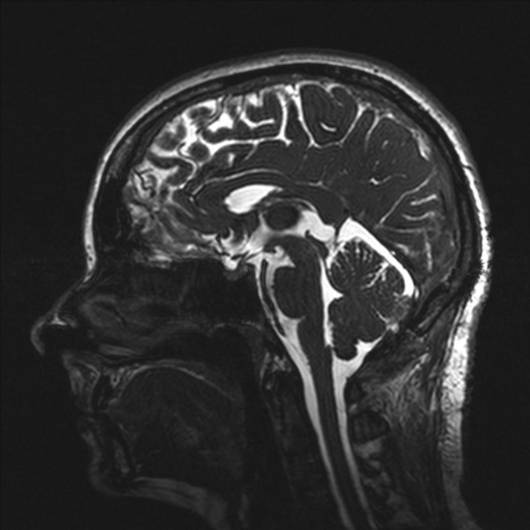
A and B: The sagittal MRI images show a large pineal cyst (arrows) that narrows the aqueduct (thick arrow).
C: Endoscopic view of the cyst.
D: Cyst opening with tenaculum forceps.
E: After cyst fenestration the cyst collapses and the aqueduct is opened (arrow).
F: View in the cyst with the pineal gland tissue.
G and H: Postoperative sagittal MR images show considerable reduction in cyst size and good cerebrospinal fluid flow through the aqueduct (arrow).
I and J: Postoperative axial MR images show considerable reduction in size of the cysts and ventricles.
The 22-year-old female patient complained of intermittent headaches, nausea and vomiting. The MRI showed a large pineal cyst that narrowed the aqueduct. The ventricles are narrow. The cyst was microsurgically completely removed in a sitting position. Since then the patient has been free of complaints.
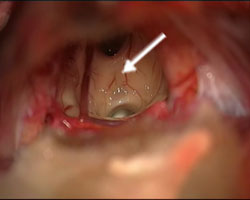
Fig. 4
A: The sagittal MRI image shows the large pineal cyst (arrows) that narrows the aqueduct (thick arrow).
B: The postoperative sagittal MRI image shows the cyst removal and the opened aqueduct (arrow).
C: Microscopic view of the cyst (arrows).
D: After the complete removal of the cyst one can see into the third ventricle (arrow).
The 38-year-old male presented with progressive headache and dizziness. MR imaging showed a large pineal cyst causing obstruction of aqueductal CSF flow and subsequent hydrocephalus.
MR imaging obtained 3 years after surgery, showed a wide cyst fenestration and confirmed restoration of aqueductal CSF flow. There is a noticeable decrease in the size of the cyst and ventricular size. The patient’s symptoms improved markedly.
The 31 years old female patient complained of headache associated with nausea and vomiting as well as double vision. MRI revealed a pineal cyst which was surgically resected.
The cyst was resected totally. Post-operative imaging revealed no complications. After 24 hours of observation in the ICU the patient was transferred to the normal ward. Three days later she could be discharged.
One year post-operatively the patient is totally free of symptoms, headache and double vision.
|