|
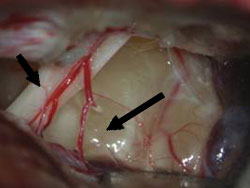
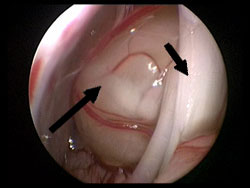
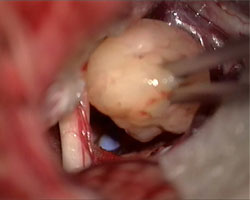
A benign tumour (Fig. 1) that arises from the Schwann cells of the sensitive facial nerve (trigeminal nerve) is referred to as trigeminal neurinoma. Since the trigeminal nerve runs in the vicinity of the vestibular nerve, auditory nerve (cochlear nerve) and the motor facial nerve, the tumour often compresses these nerves through slow growth.
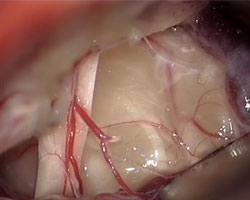
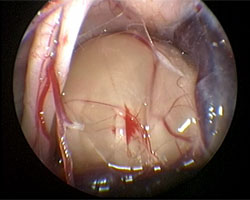
Fig. 1 Microscopic (A) and endoscopic (B) image of trigeminal neurinoma. In front of the tumour one can see vestibular nerves (short arrow), on the tumour fibres of the sensitive facial nerve (long arrow).
Most often the tumour causes numbness in the face or facial pain (trigeminal neuralgia). In the case of larger tumours that impact on the vestibular nerve-auditory nerve group, slowly progressive hearing impairment and rotatory vertigo can also occur. Facial paralysis manifests only very late. Giant tumours occasionally lead to blockage of cerebrospinal fluid pathways resulting in retention of cerebrospinal fluid and the development of hydrocephalus. The typical symptoms are then nausea, vomiting and later consciousness disturbances.
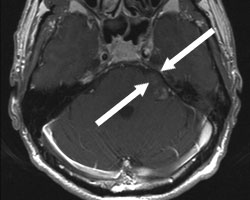
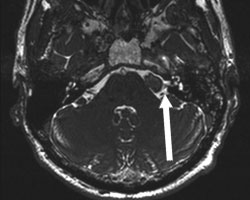
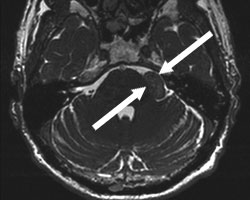
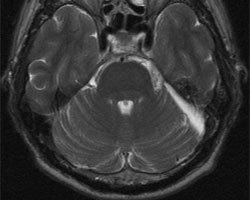
Magnetic resonance imaging (MRI) with injection of contrast agent is the examination of choice (Fig. 2). This technique permits the visualization of even very small tumours. With the CISS (constructive interference in steady-state) sequence one can depict individual cranial nerves in the cerebellopontine angle and the auditory passage, and very accurately recognize the connection of tumours to other nerves. Apart from the imaging an ENT interview for examination of hearing and equilibrium in the case of corresponding symptoms can take place.
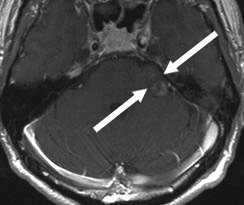
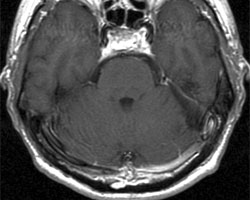
Fig. 2 MRI of trigeminal neurinoma.
A: The T1 weighted imaging shows the tumour, poorly absorbing contrast agent, in the cerebellopontine angle (arrows).
B. The CISS sequence shows the tumour expansion and the contact with the vestibular and auditory nerve (arrow).
There are basically three alternatives:
1. follow-up with regular MRI examination,
2. microsurgical tumour removal,
3. radiotherapy (radiosurgery).
In older patients and small tumours that hardly cause afflictions, the sensible option is observation of the tumour by MRI scans at semi-annual to annual intervals. In younger patients the indication for surgery is more easily set. In particular, in the case of smaller tumours there is a very good chance to remove tumour without permanent neurological disturbances. Large tumours (> 3 cm) should definitely be operated on because radiotherapy often cannot prevent further growth, and the later necessary surgery is clearly more serious due to distinctive adhesions. We recommend endoscopic-assisted microsurgical tumour removal under auditory monitoring and facial nerve monitoring. By monitoring the functional state of the auditory nerve and facial nerve is controlled.
The 57-year-old patient complained of numbness in the left half of the face. The MRI showed approx. 2 cm large trigeminal neurinoma. Via a small, approx. 2 x 2.5 cm opening in the skull (craniotomy), the tumour was revealed in the cerebellopontine angle. Under microscopic and endoscopic visual control the tumour could be completely removed. Hearing was maintained. The numbness in the face completely resolved.
Video 1 (3.2 MB)
Click to start the video.
Fig. 4
A and B: The MRI images show the tumour in the cerebellopontine angle (arrows).
C: Tumour under the operating microscope visual control.
D: Tumour under endoscopic visual control.
E: Tumour removal after dissection from the fibres of the sensitive facial nerve.
F: The final inspection shows complete tumour removal with an unimpaired facial nerve (arrow).
G and H: Postoperative MRI images show complete tumour removal.
|