|
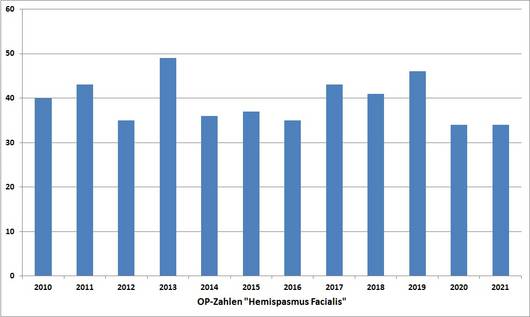
Fortunately we were able to continuously increase the number of treated patients. The graph below shows the performance development (490 surgeries between 2005 and 2021).
Hemifacial spasm is characterized by sudden, spontaneous, unilateral tonic-clonic contractions of the facial muscles. The spasms last from a few seconds to several minutes, though in severe cases they may be permanently present. In the latter cases one can often observe more or less pronounced facial palsy. There is no pain or sensory disturbances.
The cause is compression of the nerve exit zone of the motor facial nerve at the brainstem by a vascular loop (Fig. 1). Due to the permanent pulsation it leads to impairment of the nerve root (demyelination) that leads to spontaneous discharges and as a result triggers the spasms.
Fig. 1.
A: Compression of the facial nerve exit zone by a loop of the inferior cerebellar artery.
B: The close-up image clearly shows the depression that corresponds to the demyelination (arrow).
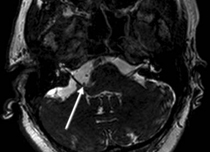
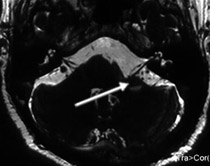
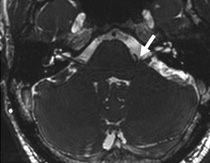
The appropriate examination in the case of hemifacial spasm is magnetic resonance tomography (MRT) with the axial and coronary CISS (constructive interference in steady-state) sequence. This sequence shows best if there is nerve compression by the cerebral artery (Fig. 2).
Fig. 2. CISS sequence with evidence of vascular compression of the right motor root of the facial nerve (arrow)
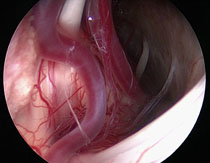
Initially, medical treatment with antiepileptics, e.g. Neurontin (gabapentin) or Tegretol (carbamazepine), is applied. In the case of persistent spasms, Botox (botulinum toxin) can be injected into the fascial muscles to suppress the spasms. If the medical treatment is unsuccessful or not tolerable because of its side effects, neurosurgical treatment provides excellent opportunities for cure with low surgical risk. If there is evidence of nerve compression by a vascular loop, microvascular decompression of the nerve is the appropriate therapy. We prefer the endoscope-assisted microsurgical technique. Under general anesthesia the facial nerve is exposed through a small opening of the skull behind the ear, then the compressing vessel is detached from the nerve root and held away with a small Teflon pledget, so the nerve is decompressed (Fig. 3). This surgery is also well tolerated by older patients (the oldest patient was 79). Microvascular decompression is a causal therapy (eliminating the cause) and provides approximately a 85% chance of permanent freedom from spasm.
Fig. 3.
A: View through the operating microscope. The vascular loop is visible in front of the brainstem (arrow). The actual compression site of the facial nerve at the exit from the brainstem is not visible.
B: View through the endoscope (70°-angled optic). Now the distinct compressions of the facial nerve can be clearly recognized at the exit from the brainstem (arrow).
C: The inserted Teflon pledget keeps the vascular loop away from the nerve and prevents it from sliding back.
The patient had complained of right hemifacial spasm for about 3 years.
Fig. 4. The CISS sequence shows a clear vascular compression of the left motor facial nerve (arrow).
In the following video the endoscope-assisted microvascular decompression is presented. The facial nerve is exposed in the cerebellopontine angle. One can observe a double compression of the facial nerve by the strong basal cerebral artery and the inferior cerebellar artery. The vascular loops are identified, dissected and kept away from the nerve with a Teflon pledget. One can see how favorable it is to use an endoscope to inspect the nerve and the compressing vessel.
[Translate to English:] Video 1.
Hemispasmus facialis (2.5 MB)
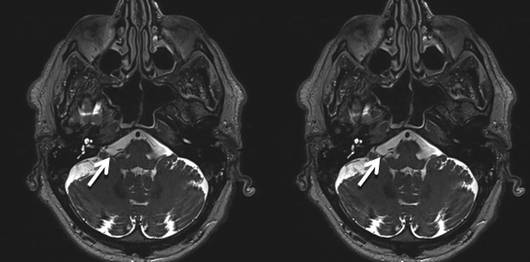
The 42-year-old patient had complained of a slowly progressive left hemifacial spasm for about 9 years. At presentation in our clinic there was an almost continuous strong hemispasm with clonic (short) and tonic (long lasting) contractions of the facial muscles (see video 2). The preoperative MRI examination (CISS sequence) clearly shows the compression of the exit zone of the facial nerve from the brainstem by a loop of the posterior inferior cerebellar artery (Fig. 5). During the surgery the exit point of the motor facial nerve is exposed under microscopic and endoscopic visual control (video 3). Now the loop of the inferior cerebral artery that compresses the facial nerve, as recognizable on the MRI images, is clearly visible (Fig. 6). After mobilization of the loop, a Teflon pledget is placed between the brainstem and the blood vessel to prevent the vascular loop from sliding back (Fig. 7). After the surgery there still were strong spasms that completely resolved only 4 months after the operation. In particular in patients who have suffered from hemispasm for many years the remission of symptoms can take a longer time since the nerve has been severely damaged by the years of compression. At presentation 8 months after the surgery, complete remission of symptoms is achieved (video 4).
Fig. 5: The CISS sequence shows a clear vascular compression of the left facial nerve (motor facial nerve) at the exit point from the brainstem (arrow).
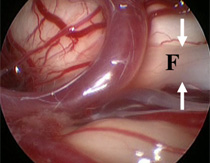
Fig. 6: Endoscopic view of the vascular loop that compresses the facial nerve (F) (the nerve is between the arrows).
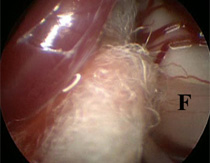
Fig. 7: Endoscopic view after mobilization of the vascular loop and insertion of the Teflon absorbent pad.
Video 2: The video shows the patient before the surgery.
Severe continuous left hemispasm can be observed. (1.3 MB)
Video 3: The video shows the endoscope-assisted microvascular decompression surgery. (2.2 MB)
Video 4: The video shows the patient 8 months after the surgery.
Complete remission of symptoms is achieved. (2.3 MB)
This 66-year-old male has complained of a permanent right hemifacial spasm for 12 years. The botulinum toxin injections were only initially effective. Prior to the operation, the patient was suffering from a severe hemifacial spasm with tonic and clonic components. The CISS sequence of the MR imaging revealed a compression of the right facial nerve at its origin from the brainstem, caused by a loop of the anterior inferior cerebellar artery.
The hemifacial spasm has completely disappeared after the surgery. The patient does not have any neurological deficits.
|