|
The term “syringomyelia” refers to a fluid-filled cavity (syrinx, Greek: tube) in the grey matter of the spinal cord (myelon). If the syringomyelia spreads up to the lower brainstem, it is referred to as syringobulbia.
The clinical afflictions often involve pain and dissociated disturbances of sensation. In various body regions independently from each disturbance of perception of pain, perception of temperature, proprioception, and also cutaneous sensibility can occur. Syringomyelia can also lead to paralyses in legs or arms.
Each case of syringomyelia has a cause. The most frequent causes are spinal cord tumours, inflammations of the spinal cord, injury of the spinal cord (trauma), vascular malformations, adhesions or adherences of the spinal cord (tethered cord) or compressions that primarily occur in the region of the junction from the skull to the spine (e.g. Chiari malformations). If one cannot find, despite extensive diagnostics, any distinct cause (this applies to approx. 20-30% of cases), it is referred to as idiopathic syringomyelia.
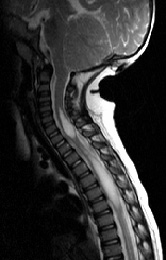
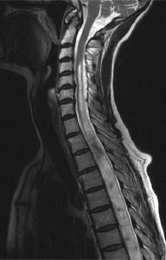
Diagnosis of syringomyelia takes place through magnetic resonance imaging (MRI). The MRI examination serves on one hand to depict cavity development in the spinal cord, but on the other hand also to search for the cause. That is why it is crucial to image the entire spinal canal, i.e. including the entire spinal cord pathway, and to carry out the examination without and with a contrast agent. A differentiated assessment of syringomyelia also includes the examination with flow-sensitive sequences in MRI. Ultimately, the formation of a syrinx is based on the fact that – also always by which cause – the fluid circulation (cerebrospinal fluid) is disturbed in the spinal canal.
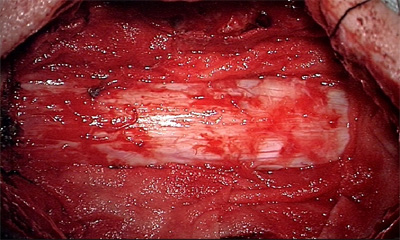
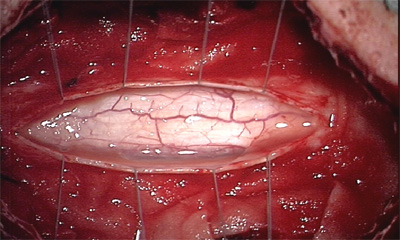
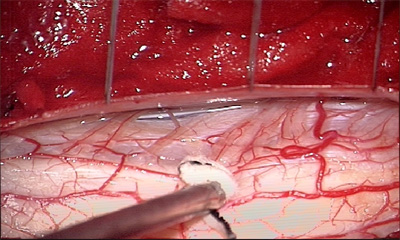
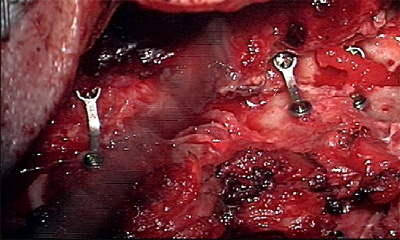
The therapy in syringomyelia consists in removing the cause. In the case of a space-consuming lesion, e.g. by a tumour, it has to be microsurgically removed. In the case of an adherence or restraint, e.g. by a tethered cord, the aim of the surgery is to microsurgically release the restraint place in order to enable the free circulation of the cerebrospinal fluid, spinal cord and nerve fibres in the spinal canal. In the case of a compression in the cranio-cervical junction, e.g. by a Chiari malformation, the therapy of choice is a decompression with extension plasty. If the syringomyelia is based in its development on adhesion or adherence in the inside of the spinal cord canal, the aim is to release this adherence microsurgically. This surgery is termed adhesiolysis. The insertion of a drainage in the syrinx is widely abandoned because it turned out that it leads in time to adherence of the catheter and the syrinx redevelops.
The aim of the syringomyelia surgery is to prevent the progression of clinical afflictions and to stabilize or resolve neurological deficits. Complete recovery is not always possible. According to morphological appearance criteria, success is achieved if the syrinx resolves partly in its dimensional extent. Complete normalization of the spinal cord cannot usually be achieved or expected. Regular follow-ups are necessary, mainly MRI, in order to exclude reoccurrence of syrinx also after the surgery.
A 70-year-old female patient suffered in early adulthood from a serious road accident with a fracture of the vertebral body and paraplegia. Over several years increasing pain as well as paraesthesia and weakness (paresis) developed in the previously completely unaffected arms, in particular in the region of the hands. The MRI imaging showed a cranial ascending syringomyelia starting from the region of the former fracture of the vertebral body. The therapy was to release arachnoidal adhesions in the area of the former site of injury as well as in a microsurgical opening of the syrinx. After the surgery the pain and paresis in the arms largely receded.
|