|
The term “Chiari malformation” derives from the name of Hans von Chiari (1851–1916), who described it first. Chiari while the full professor for Pathological Anatomy at the University of Prague in 1891 described various changes of the cerebellum that were mainly associated with hydrocephalus. In the original classification four Chiari types were described. Currently clinically relevant are Chiari malformation types I and II.
Caudal displacement of cerebellar tonsils, max. up to the top edge of the 2nd cervical vertebra. The malformation is assumed to be congenital. The clinical symptoms develop earlier in young adulthood up to the age of 30 and consist mainly of headaches in the back of the head region that can increase motion dependently and stress dependently. Further symptoms are paraesthesia in the arms and legs and pain in the area of the cervical spine, but also paralyses, e.g. hemiparalysis, can occur. Chiari I malformation is sometimes associated with the formation of syringomyelia.
Caudal displacement of cerebellar tonsils to the region of the middle cervical spine (C2–C4). Chiari II malformation is generally identified by a caudal displacement not only of the cerebellar tonsils, but also of the brainstem, of the 4th ventricle and of the upper medulla oblongata (upper spinal cord). The posterior cranial fossa has small anatomical dimensions and the confluence of sinuses (vein junction of the large skull veins) is displaced far beyond caudally. Chiari II malformation is almost always accompanied by the presence of spina bifida, i.e. arch closing malformation of the vertebrae, usually in the lumbar area. As a result patients with Chiari II malformation often have to be surgically treated due to spina bifida. In approximately 80% of patients also hydrocephalus requiring treatment is present. Additionally Chiari II malformation can be associated with syringomyelia.
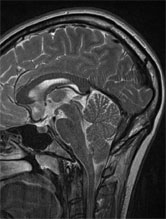
The diagnostic method of choice is magnetic resonance imaging. First of all it is possible here in T2-weighting to assess anatomical variants as well as the grade of the compression of the spinal cord in the foramen magnum. Furthermore, MRI associated changes (e.g. conus low-level, syringomyelia, tethered cord, hydrocephalus) can be recognized. The recording of somatosensory evoked potentials (SSEPs) serves as electrophysiological supplementation for magnetic resonance tomography.
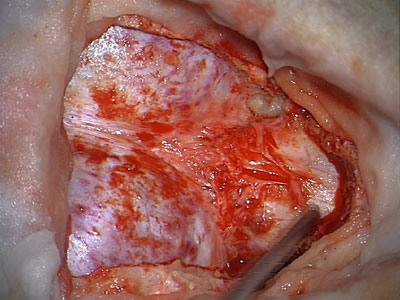
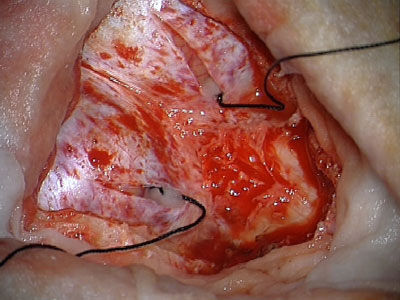
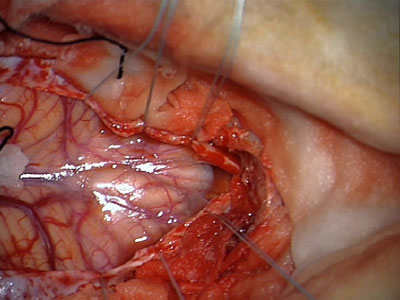
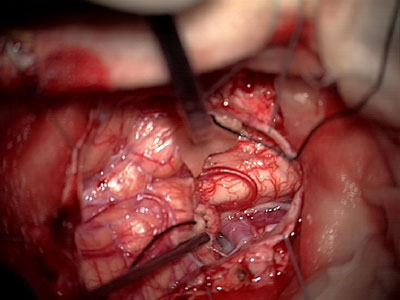
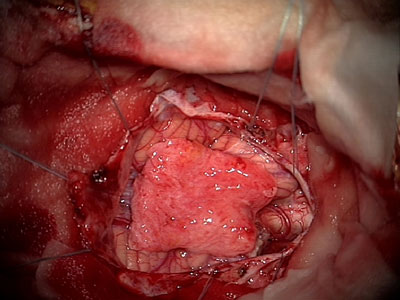
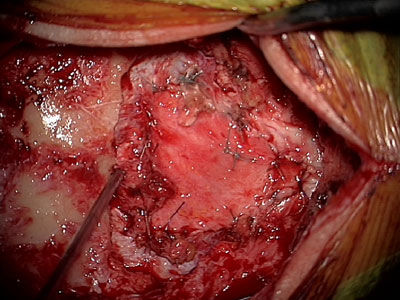
The therapy of choice consists in making a decompression in the region in which the cerebellar tonsils in the spinal canal compress the upper spinal cord and the lower brainstem. This happens through a suboccipital craniectomy (bone removal in the region of the back of the head). Due to this action a bony passage from the brain to the spinal cord is extended. As a rule laminectomy (removal of the vertebral arch) for the 1st cervical vertebral body and in Chiari II malformation also possibly for the 2nd cervical vertebral body is carried out. Also this serves for bony decompression. After sectioning or separating external membranes or adhesions associated with the dura mater of the brain or spinal cord, the dura matter is opened. The cerebellar tonsils are mobilized and freed from potential arachnoidal adhesions and adherences. The aim is to rebuild a free fluid flow from the 4th ventricle in the spinal canal, but also in the region of the subarachnoid space. In some cases microsurgical partial resection or resection of one of the cerebellar tonsils is necessary. After sufficient internal decompression a dura vasodilating plastic material is finally stitched onto the open dura mater of the brain/spinal cord. Also this action serves to vasodilate the passage from the skull to the vertebrae or the passage from the brain to the spinal cord where there is the Chiari malformation. The duraplastic material is preferably made from the body’s own material that is obtained during surgical access (e.g. periosteum). In rare cases it is necessary to use a dura replacement preparation.
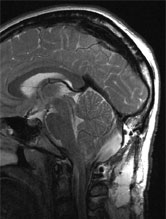
A 28-year-old female patient presented with right-sided headaches that increased considerably in the course of a few weeks. Parallel to this developed hemiparesis (hemiparalysis). After carrying out extensive neurological and imaging data diagnostics Chiari I malformation with low-level tonsils and compression of the upper spinal cord was diagnosed. During the decompression surgery widening of the foramen magnum, as well as C1 laminectomy (removal of the vertebral arch), was performed. After opening the dura mobilization of the cerebellar tonsils and tonsil resection took place. After establishing a free nerve fluid flow from the 4th ventricle in the spinal subarachnoid space the duraplastic material was made from the body’s own material and stitched on watertightly. The hemiparesis and pain in the back of the head resolved after surgery.
Fig. 3: Left: MRI at sagittal level before surgery, right: postoperative MRI, behind the cerebellum and in the foramen magnum a clear fluid signal is visible now.
|