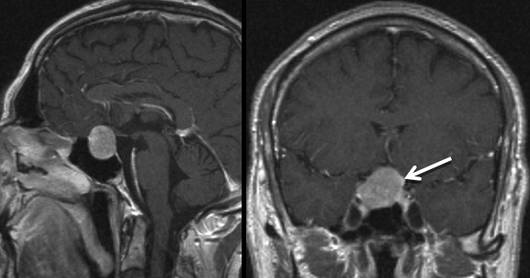
The 54-year-old patient presented with loss of libido and erectile dysfunction. He also reported a narrowed visual field. The endocrinologic diagnostics determined a partial insufficiency of the somatotropic and gonadotropic anterior pituitary axes. MR imaging identified the cause as a homogeneously enhancing intrasellar and suprasellar lesion. The size of the tumor meant that the optic chiasm was already considerably elevated and appeared flattened. The pituitary gland and pituitary stalk were displaced to the left. After careful assessment of all the diagnostic findings, a non-secreting pituitary adenoma was suspected.
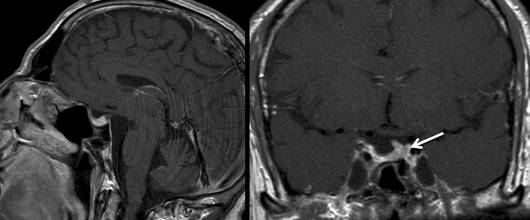
The patient recovered excellently after the surgery. His visual field returned to normal. One year after the operation there were neither clinical nor laboratory findings to suggest pituitary insufficiency, so the replacement therapy was stopped. The MR imaging performed one year after surgery showed complete removal of the tumor with a well defined remaining pituitary gland in the left corner of the sella and normal conditions in the paranasal sinuses.