|
The lumbar area is subject to significant stress. This may lead to pathological distribution of weight and even more stress, especially in the lower part of the lumbar spine, resulting in pain and/or functional disorders of the nerves.
The simplest form is disc protrusion. The disc pushed out of its natural position can cause low back pain (lumbago) and/or pain radiating to the legs (lumbago-sciatica).
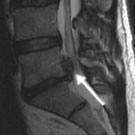
If the outer, fibrous ring of the intervertebral disc tears the soft central portion of the disc bulges out into the spinal canal. The clinical manifestation often includes very severe back pain. If the protruding disc compresses the roots of spinal nerves lumbago-sciatica symptoms may occur, including sensory changes, ranging from numbness to paralysis of the legs or gluteal area. In cases of massive herniation nerve fibres innervating the bladder or rectum may also be severed. This serious and luckily seldom occurring condition is accompanied by urinary and bowel incontinence and requires immediate emergency treatment in a specialist clinic.
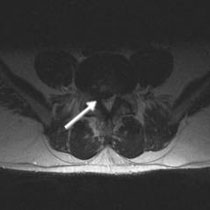
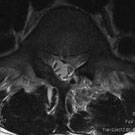
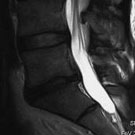
Fig. 1. Cervical disc herniation at the level of 4th and 5th lumbar vertebrae on the right side. Magnetic resonance image (transverse left, right sagittal transsection)
The focus of the treatment is conservative physical therapy. It aims at increasing the strength of usually neglected abdominal and back muscles using various techniques. Pain can be managed using analgesic medication. The so-called step bed position can also bring some relief – the patients are trained to find and assume an adequate body position which decreases the pressure on the disc, at the same time reducing the irritation of the nerve roots. Application of heat in the form of a bath or mud bath (mud packs) can also be helpful.
However, the most important element of physical therapy in these cases is an adequate exercise programme, which enables patients to actively relax their back using selected groups of muscles. Most patients benefit significantly from physical therapy measures, thus avoiding the need for surgical treatment.
Conservative treatment can be applied both in outpatient and inpatient settings. The patient's motivation is crucial for the success of this treatment. Physical therapy helps patients to help themselves. Long-term relief is possible only if the patient consequently continues to exercise at home according to received instructions.
Anamnesis – medical history of a patient is an essential element of the diagnostic process. Information obtained from a patient may point to the source and location of the problem. Physical examination is another crucial step, often enabling the physician to locate precisely the level of the herniated disc. Additional tests complement the diagnostic process.
Commonly used tests include: - Magnetic resonance imaging (MRI): the method of choice for imaging of spinal cord, nerve roots and intervertebral discs
- X-ray of vertebral column may help diagnose malformations, deformities and severe degenerative changes of the spine
- Functional imaging of vertebral column for diagnosing its instability
- Computed tomography scan (CT or CAT) for visualisation of the bone structure of the vertebral column
- In cases of contraindications against MRI (for example cardiac pacemakers, old metal implants) a CT myelogram may be necessary (computed tomography image obtained after radiography contrast media has been injected into the spinal canal fluid)
- Electrophysiological tests can be used to locate the site of nerve lesion
- Discography – an imaging procedure used to determine which discs are causing pain
Immediate emergency surgical treatment is necessary in cases of massive disc herniation with severe narrowing of the spinal canal leading to urinary or bowel incontinence. Delay of surgery may lead in such cases to permanent functional deficit.
Cases of suddenly occurring paralysis also require immediate surgical intervention. Delay may also result in permanent lesions.
Chronic, treatment-resistant pain not responding to adequate physical treatment is also an indication for surgery. - Microsurgical operations on intervertebral disc
- Minimally invasive spine surgery using muscle dilatators
- endoscopic spine surgery
This technique comes into play in cases of extensive wear-induced changes affecting the vertebral column, with enlargement of intervertebral joints and ligaments, narrowing of the spinal canal due to bone damage and in cases of repeated surgical treatment.
The critical site is accessed through a skin incision measuring 3-4 cm, allowing the removal of bone and ligament tissue causing the narrowing of the spinal canal, as well as decompression of nerve roots. In some cases loose, significantly degenerated parts of intervertebral disc nucleus also have to be removed. In most cases however, the disc itself can remain in place, allowing preservation of mobility of the spine in the affected area.
This technique uses a small, 15 mm long skin incision with a canal allowing access to the site of interest. The intervertebral disc hernia is then removed under high magnification. Due to the small incision and minimal stress for the muscles the postoperative pain is significantly reduced. Similarly, no significant blood loss occurs. Since the postoperative trauma is minimal patients are able to get up from bed on the day of surgery and their discharge from the hospital may soon follow.
Fig. 2. Instruments for minimally invasive surgical technique
Fig. 3.
A: Dilatation of transmuscular access with access tubes of varying size
B: Surgery through a tubular retractor system with diameter of 14 mm
Fig 4. X-ray control image to ensure that the tubular retractor is in the correct position (arrow points to the intervertebral disc)
Fig. 5.
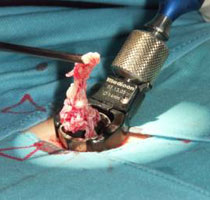
A: Removed disc hernia held in forceps
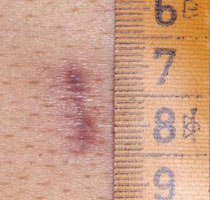
B: Postoperative 15 mm long scar, 2 months after surgery
Fig. 6.
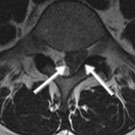
A and B: Magnetic resonance image (MRI) obtained from a patient with severe lumbago-sciatica and peroneal nerve palsy on the left side. A sequestrated disc prolapse between lumbar 5 and sacral 1 vertebrae is visible (arrows)
C: Postoperative CT scan; minimally invasive access (8 mm wide opening in the arch of the vertebra) to the herniated disc.
D and E: Postoperative MRI scan showing complete removal of disc herniation. The patient was symptom-free directly after the surgery. The paralysis of his foot resolved completely in the follow-up period.
Endoscopic surgery is used mostly in cases of disc herniation in the area of the neural foramen (the bony openings in the spine that allow the nerves to leave the spinal cord). The procedure is performed under local anaesthesia and concomitant analgesic medication. The disc herniation can be removed through a very small incision with endoscopic control of the whole procedure.
Fig. 7.
A: Placement of the guiding needle for endoscopic disc surgery in the lateral position
B: X-ray image at two levels to control the position of the surgical approach
Fig. 8. Surgery in process with endoscope in working position
With the assistance of our physiotherapists patients can get up already on the same day the operation has been performed. The hospital stay is relatively short. During the postoperative phase the patients are trained in basic behavioural rules and exercises to strengthen and protect their spine. They should continue to exercise after discharge from our clinic, in cooperation with their family doctors. Subsequent rehabilitative treatment is recommended. Should you need any advice on that topic, our social workers will be glad to answer your questions.
Complications after this procedure are relatively rare. If unexpected problems do occur during or after surgery, they can usually be quickly and reliably resolved in cooperation with a maximum care hospital. Your attending physician will give you detailed information on that matter.
|