|




|
|
|
|
|
|
|
 |
|
|
|
|
|
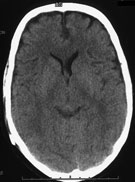
Hydrocephalus refers to the situation when the fluid volume (cerebrospinal fluid) increases at the expense of brain volume.
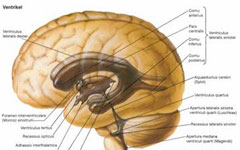
The fluid forms first of all in the ventricles, in the choroid plexus. There are 4 ventricles in the brain that communicate with each other via the foramina and aqueduct. The cerebrospinal fluid also bathes the exterior of the brain and spinal cord, and then is delivered into the blood stream. Formation and drainage of the fluid are in balance with each other. If this balanced relation becomes disturbed, hydrocephalus develops.
If the fluid is blocked, the pressure increases. The ventricles increase in size, the brain tissue is under tension and as a result the brain circulation and oxygen supply are impaired. In small children up to the age of one year the increased fluid pressure has an effect on skull growth (increase in size of the head), since the cranial bones are pushed apart.
Signs of cerebral pressure: - Headache, neck pain (at first usually in the morning)
- Nausea, vomiting (at first morning dry vomiting)
- Vision disorders (papilloedemas, double vision)
- Tiredness, consciousness disturbances, seizures
- In infants unrest, changed drinking behaviour, persistently shrill scream, tense fontanelles
HAKIM trias: (typical in normal pressure hydrocephalus)
- Walking disorders (small steps, feet placed wide apart, weak legs)
- Dementia and character changes (forgetfulness, becoming slower, greater irritability)
- Bladder and stool incontinence
Other symptoms:
- Parkinson’s symptoms
- Ocular motility disturbances (cross-eyes, “setting sun sign”, malfunctions of visual field), deterioration of acuteness of vision up to loss of sight
- Problems of hand-eye coordination with fine motor skill disturbances
- Vertigo, drop in performance, concentration disturbances
- Development of learning disability in children
- Changes of personality, behavioural syndromes (unrest, aversion, impatience), hyperacusis
- Breathing trouble, speech trouble, difficulties in swallowing
- Endocrinological disturbances (metabolic disturbances), premature puberty before the age of 8 (very rare)
- Disturbances of the fluid circulation through passage obstructions (cysts, tumours, haemorrhages) = obstructive hydrocephalus
- Disturbances of fluid absorption (inflammation, haemorrhages, brain injuries)
Hydrocephalus can also be congenital. The causes include developmental disorders in the womb (spina bifida, neural tube defect), Chiari malformation (malformation of brain structures of the posterior cranial fossa) or Dandy-Walker syndrome (cystoids transformations in the region of the 4th ventricle and the cerebellum). Also infections in pregnant women can cause the development of hydrocephalus in the fetus. Hydrocephalus can also develop in consequence of cerebral haemorrhages in premature babies (delivery before the 32nd week of pregnancy, birth weight below 1000 g).
Hypersecretory hydrocephalus | Surplus production of cerebrospinal fluid | Malresorptive hydrocephalus | Absorption disturbances of the cerebrospinal fluid
 | Occluded hydrocephalus | Occlusion of fluid paths | Communicating hydrocephalus | no relocation of fluid paths, absorption disturbances
| Internal hydrocephalus | Expansion of internal fluid cavities | External hydrocephalus | Expansion of external fluid cavities | Hydrocephalus ex vacuo | Atrophy (depletion of brain mass)
| Active hydrocephalus | Hydrocephalus with increase of pressure |
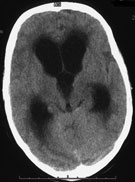
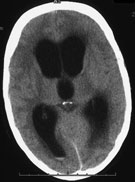
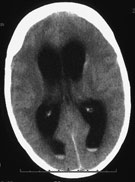
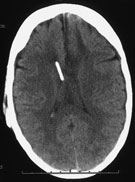
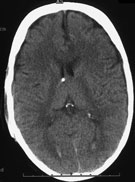
- Computed tomography
(incorrectly expanded system of cerebral ventricles, frontally stressed density decrease in ventricle vicinity = “pressure caps”, flattened brain furrows) - Magnetic resonance imaging (shows possible causes such as tumours, sedations, cysts, constrictions or occlusions)
- Intracranial pressure monitoring (measurement of pressure in brain through probes)
- Ultrasound (effective and convenient to carry out in children through fontanelles or thin cranial bone, because there is no exposure to X-rays, determination of ventricle width and follow-ups very possible, causes of hydrocephalus can be shown)
- TAP-Test = fluid drainage test (through a lumbar puncture = taking 30-50 ml of cerebrospinal fluid from the vertebral canal, afterwards the patient is neurologically examined, in particular the gait is tested)
- Infusion test (through a change of volume by adding fluid from outside in the fluid system the adaptability of the system to changed volumes and pressures is tested)
- Other examinations (neuropsychological tests, cerebral ultrasound)
Untreated hydrocephalus leads to severe functional neurological deficits because of the irreversible impairment of nerve cells. In rare cases there is a danger to life.
If possible, the cause of hydrocephalus (e.g. brain tumour) is surgically removed. Currently there is no effective medication that has a long-term effective influence on fluid production.
Theoretically there are two possibilities of surgical therapy:
- Endoscopic third ventriculostomy (ETV):
the floor of the third ventricle is opened using an endoscope and catheter in order to create collateral circulation for the fluid within the ventricle system. An indication for surgery is obstructive hydrocephalus.
- Implantation of the shunt system:
A shunt consists of a catheter (tube) that is inserted in the ventricular system. The catheter is connected with a valve that regulates the fluid drainage. A further catheter then follows that ends in the abdomen under the peritoneum or in the right atrium, and drains the cerebrospinal fluid. This procedure is applied in communicating hydrocephalus (disturbances of fluid absorption).
- External ventricular drain or lumbar drain:
It is only used as a temporary treatment method in sudden circulation disturbances.
|
|
|
|
|
|
|