Little attention has been paid to injuries of peripheral nerves. For the affected patient each disturbance of a motor function and/or sensitivity of the diseased limb means a considerable impairment that can involve serious practical loss in professional as well as personal terms (quality of life).
Nerve lesions are to be found first of all in the upper limbs, and in particular in injuries of the hand. The ulnar nerve itself is involved in about 30% of cases. Traumatic peripheral nerve lesions can arise in various circumstances (sports injuries, road accidents, iatrogenic injuries, occupational accidents, explosions, etc.). Sharp or blunt force traumas can be a possible cause of peripheral nerve injuries. Also nerve traction can occur through joint luxations or fracture dislocations.
The fact that approx. 5% of all open wounds on limbs are complicated by peripheral nerve injuries emphasizes the importance of therapy optimization.
The need for adequate treatment of such injuries favours the application of microsurgical techniques and the logistics for primary and secondary care of seriously injured patients. Apart from these available therapeutic possibilities, above all the experience of the surgeon and knowledge about possible grades of nerve lesions and stages of fibrotization are relevant and both the selection of a suitable moment for surgical care and the selected surgical method for nerve regeneration are crucial. One cannot expect sudden elimination of functional disorders. The symptoms of nerve injury may resolve for example only after many months after the nerve grafting. The nerve grows from the site of injury to a different cut end approx. 1 mm per day.
A further crucial aspect with regard to the success of treatment is the patient’s motivation in the course of a very lengthy aftercare.
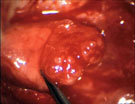
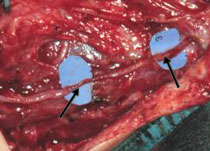
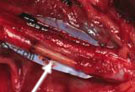
After a fresh open nerve lesion due to cutting or stabbing injuries, if possible a quick primary nerve suture (Fig. 1) is made (secondary nerve suture, see Fig. 2).
The nerve suture is, if possible, to be aimed at, because the functional results after the nerve injury deteriorate with passage of time. The condition is a tension-free adaptation of both nerve endings.
If the nerve suture is not possible, early secondary treatment within 4-6 weeks after the primary wound repair is aimed at.
Closed nerve injuries (blunt trauma) with complete or serious neurological deficits without evidence of spontaneous reinnervation (clinical and electrophysiological) within 3 months after the injury are also indications for surgery. Depending on the intraoperative findings either microsurgical neurolysis (Fig. 3) (epineurotomy, epineurectomy), neuroma resection with subsequent nerve suture or a free interfascicular nerve grafting is performed (Fig. 4 -6).
All operations are carried out using microsurgical techniques.
The sural nerve is inserted most often as the nerve graft. It is typically taken via multiple transverse incisions on the parietal lower leg. But also the great auricular nerve, as well as the transverse cervical nerve and supraclavicular nerves, serve in some cases as autologous nerve grafts.
In the case of an end-to-end suture it is attempted to re orientate the cut nerve ends so that the bundles of nerve fibres (fascicles) fit exactly on top of each other. The blood vessels in the conjunctive tissue of the nerve help here in orientation.
Fig. 1: Nerve suture
A: Nerve stump with 2 fascicles (arrow)
B: Stump preparation
C: Epineural suture
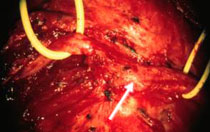
Fig. 2: Lesion of ulnar nerve in the region of the left elbow. The patient fell from a bicycle and sustained a supracondylar humeral fracture that was treated with Kirschner wire osteosynthesis.
A: The nerve (marked yellow) ends in a large ganglion (neuroma, arrow).
B: After excising the neuroma a suture of the nerve end after gaining length was achieved under the musculature by displacing the ulnar nerve forward.
C: Pronounced paralysis in the hand region (typical “claw hand”) with muscular atrophy as a result of nerve injury (ulnar nerve) before surgery.
D: Complete remission of the hand paralysis and muscular atrophy. It is possible again to splay out the little finger.
In the course of this the nerve is liberated from the binding fascial tightness.
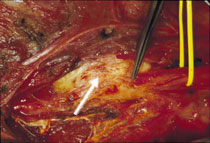
Fig. 3: Paralysis of the radial nerve after osteosynthetic treatment of humeral fracture.
A: Intraoperative findings. The nerve is compressed by a massive bone formation (arrow, the radial nerve is marked with a yellow line).
B: After carrying out neurolysis the nerve lies relaxed.
C: Clearly limited stretching in the wrist and stretching of fingers before surgery.
D: Very good recovery of the extensor muscle deficiency after surgery.
If the denervation was not directly provided both endings of the injured nerve retract from the site of injury. After a few weeks the gap is already so large (a few centimetres) that direct suture is not possible any more. Between the two endings forms the so-called ganglion (neuroma), which can be very painful. Now the conduction of the nerve grafting for the nerve reconstruction is required. In the course of this the neuroma has to be removed. The nerve defect that occurs in doing so is bridged by a donor nerve. During that the nerve tissue is taken from the injured person. The donor nerve comes most often from the sural nerve that runs at the outer edge of the foot and lower leg.
Usually the transverse incision of the injured nerve is greater than the one of the donor nerve so further donor nerve fractions are necessary to cover the transverse incision. The stitching of the nerve grafts for bridging the defect takes place under the microscope with the help of very small sutures hardly visible to the naked eye. On the basis of the newly created guide sheath newly growing nerve fibres can now bridge the defect.
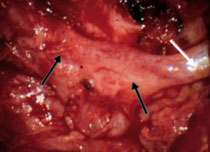
Fig. 4: Common fibular nerve lesion in the region of the right hollow of the knee. The patient was attacked by a shot boar and bit in the right hollow of the knee while hunting. The nerve was ripped. A: The common fibular nerve (marked with a yellow line) ends in a ganglion (neuroma, arrow).
B: Bridging the defect with several nerve grafts (sural nerve, arrow) after resection of the neuroma.
C: Complete paralysis of foot lifting (on the right) before surgery.
D: Already extensive remission of the right foot lifting deficiency 24 months after surgery.
Fig. 5: Patient with accessory nerve paresis in status post lymph node removal in the lateral left cervical region.
A: It turned out intraoperatively that the nerve ended in a large cicatricial mass. The distal nerve stump was found only approx. 2 cm distally further (cicatricial mass, margin marked by black arrows; white arrow marks the accessory nerve).
B: Bridging the defect with a nerve graft (great auricular nerve; marked with arrows between the blue markings) after resection of the cicatricial mass.
C: Deficiency in shoulder lifting and atrophy of the left trapezius muscle before surgery.
D: Complete remission of paralysis. Left shoulder lifting possible again (1 year after surgery).
Fig. 6: Partial median nerve injury after fall into a glass door with a deep cut in the region of the left middle upper arm. The nerve injury was not described during the first care of the patient in an out-of-town hospital. The patient had incomplete paralysis of the median nerve with typical “oath hand” and sensory disturbance, mainly in the forefinger and middle finger.
A: It turned out intraoperatively after nerve liberation that the described nerve half was distended. The distension (arrow) refers to a ganglion (neuroma).
B: Further preparation of the nerve (epineurotomy). A large bundle (nerve fibre) that builds the neuroma is separated away from the other – completely intact bundles. The neuromatously distended bundle cannot be stimulated and because of that it is resected. (The arrow indicates intact nerve fibres, next to the neuromatously distended bundle).
C: The defect (1.5 cm) is bridged by stitching two nerve grafts (medial cutaneous nerve of forearm) (arrow).
D: Fist clench; E: Key pinch grip; F: Pinch grip possible again 3 years after surgery because of complete remission of paralysis.
After nerve grafting surgery immobilization with gypsum plaster for 10 days takes place; after primary stitching for 3 weeks.
In order to prevent hyperextension of muscles, preoperatively (e.g. in drop hand) immobilization with a splint is applied.
The crucial aftercare is based on intensive physiotherapy with active and passive exercises and ergotherapeutic activities, as well as stimulation current treatment (exponential current) of the denervated musculature. In median nerve injuries aesthesia training is additionally carried out.
After about 3 months a follow-up visit in our neurosurgical outpatient department takes place with an investigation of the neurological status and updated electromyogram (EMG).
Apart from the care of individual injured peripheral nerves also the treatment of complex nerve injuries in the plexus region (brachial plexus) – that often occur after accidents, and in particular after motorbike accidents – is carried out.
Reconstructive surgery or replacement surgery (e.g. free muscle transplantations, sinew transfer or muscle transfer) is possible in the case of lack of success.
|