The affected nerve (ulnar nerve) runs in the elbow region in a narrow bony groove that is referred to as the ulnar nerve groove (at this place, for instance because of an impact, an electrifying pain can be triggered; “funny bone”). This groove is covered by a tight connective tissue. If in this already narrow area an additional space-consuming lesion occurs (e.g. through bony formations, after bone fractures or a tumour), the nerve is damaged due to increased pressure.
The patient complaints of sensation disturbances in the region of the ring finger and little finger as well as the side of the hand. If the injury continues for a longer time, a paralysis of the small hand muscles right up to the occurrence of a typical claw hand as well as muscle atrophy in the hand region can occur.
Fractures (bone fractures) at the cubital joint. Luxations of the ulnar nerve from the sulcus. Bone changes (osteoarthritis), bone cysts, acromegaly, cicatricial changes after injuries, ganglia, nerve tumours and soft part tumours. Also late-onset paresis (after years or decades) after late elbow fractures or luxation are known. Often no triggering cause is identified.
The description of the complaint and clinical examination of the patient are crucial. The electrophysiological examination (ENG/EMG) can confirm the suspected diagnosis.
The multiplicity of causes permits no uniform recommendation for surgical procedure.
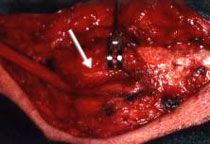
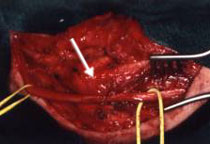
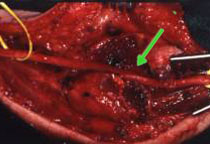
At the inside of the elbow an incision of approx. 4 cm is made (Fig. 1A). Then the division of the ulnar sulcus takes place to decompress the ulnar nerve (Fig. 1B). Usually this intervention is sufficient to achieve the “liberation” of the nerve from its straits. However, in some cases dependent on the intraoperative finding or the second-look surgery, also a displacement and new nerve embedding forwards under adipose tissue or musculature (Fig. 2 A-C) in microsurgical technique is essential. The skin incision has to be extended in order to immobilize the nerve without tension.
Fig. 1: Neurolysis of the ulnar nerve in ulnar sulcus
A: Incision on the inside of the elbow (approx. 4 cm long)
B: Division of the ulnar sulcus for decompression of the ulnar nerve
C: Subcuticular skin suture (approx. 4 cm long)
D: Subcuticular skin suture
Fig. 2: Submuscular transposition of the ulnar nerve
A: Neurolysis of the ulnar nerve in the ulnar sulcus (arrow: medial epicondyle of humerus)
B: Long exposure to proximal and distal
C: tension-free mobilization and displacement from the ulnar sulcus to ventral
D: nerve displacement under flexor musculature (arrow: newly created “bed”)
Removal of the drainage on the 1st day after surgery with a bandage change. After 10 days stitches are taken out. In the case of ensuing nerve displacement the arm is immobilized in a bent position for 10 days in gypsum plaster. Neurolysis alone does not require any special immobilization.
In pre-existing nerve deficiencies physiotherapy combined with ergotherapy should be implemented in order to rebuild the hand functionality. This can last several months, depending on the severity of deficiencies.
|