|
Trigeminal neuralgia (trigeminus = one of the nerves of the face, neuralgia = neuropathic pain) is characterized by episodes of sudden, extremely intense, one-sided pain of the face, usually in the cheek and jaw. The forehead is rarely affected. The attacks of pain can be triggered by touching, chewing or talking. Pain attacks usually last from several seconds to several minutes. Longer lasting pain with sensory symptoms is rather atypical for this disorder.
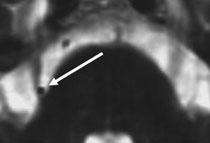
In about 90% of cases the symptoms are caused by compression of the nerve by a looped blood vessel in the area of the nerve's entry to the brain stem (Fig. 1). The remaining 10% are caused by other factors, such as tumours, inflammatory diseases, and multiple sclerosis.
Fig. 1. Compression of the trigeminal nerve by a loop of the superior cerebellar artery (arrow).
In typical cases of trigeminal neuralgia magnetic resonance imaging is the diagnostic method of choice (axial and coronary CISS sequences – constructive interference in steady-state). This procedure allows one to find out if the brain artery compresses the nerve (Fig. 2). At the same time other potential causes (e.g. tumour) can be excluded. In cases of trigeminal neuralgia associated with inflammation of sinuses or dental disorders patients need to be examined by a laryngologist or dentist, respectively.
Fig 2. CISS sequence showing compression of the right trigeminal nerve root by a blood vessel (arrow)
First-line treatment is anticonvulsant medications, with Neurontin (gabapentin) as a leading pharmacological agent. In the case of unsatisfactory effects of medication or intolerable side-effects, neurosurgery may offer highly effective treatment, associated with minimal risks of complications.
If there is evidence of nerve compression by a vascular loop, microvascular decompression is the treatment of choice. We prefer the endoscopic-assisted microsurgical technique. It is performed under general anaesthesia through a small bony opening behind the ear. During this procedure the blood vessel compressing the nerve is displaced and fixed away from the point of compression using a small Teflon implant (Fig. 3). This operation is generally well tolerated, including by senior patients (our oldest patient was 87). There is an approximately 85% chance of permanent pain relief following this surgery. In patients with serious concomitant disorders and high risk associated with general anaesthesia glycerol injections into the Gasserian ganglion can be performed (nerve loop at the base of the skull), with ca. 80% chance of immediate pain relief. However, cases of relapse of pain attacks are significantly higher after this method (ca. 40% relapses in 5 years) compared to microvascular decompression.
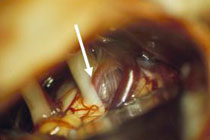
Fig 3.
A: View through the operating microscope. The vascular loop compressing the nerve is visible (arrow).
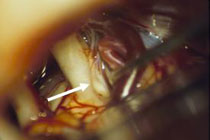
B: The vascular loop is separated from the nerve. Indentation in the nerve through years of compression (arrow)
C: Video: Endoscopic view of the vascular loop compressing the nerves at the point of their entry into the brain stem. (Click the video to start watching).
D: Teflon implant between the nerve and the vascular loop
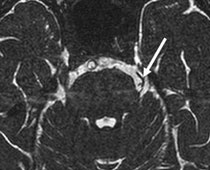
The patient had suffered from left sided trigeminal neuralgia pain attacks for the last 12 years.
Fig. 4. The CISS sequence shows a clear vascular compression of the left trigeminal nerve (narrow).
The following video shows the endoscopic microvascular decompression procedure. The nerve is freed in the area of the cerebellopontine angle, then the vascular loop is identified, separated and permanently fixed away from the nerve by a Teflon implant. One can see the advantages of the endoscopic procedure, characterized by quick and unequivocal identification of the affected nerve and compressing artery.
Immediately after the surgery the patient was pain-free. All pain medications could be stopped. Three years after the surgery the patient remains free of symptoms.
|