Brain tumours include all tumours inside the cranium (skull). The most common types of brain tumours are meningiomas (tumours of the meninges) and gliomas (tumours of the glial cells of the brain). Cancers located primarily in other organs can spread to the brain, causing typical brain tumour symptoms (metastatic tumours).
Brain tumours can cause various clinical symptoms. The pressure or infiltration caused by them on some brain areas may lead among other things to seizures, paralysis of the limbs, speech and/or visual impairment. Tumours that grow to a certain size cause intracranial hypertension, usually associated with headache, nausea, vomiting, and later also altered state of consciousness. Untreated, tumour growth leads eventually to death caused directly by paralysis of breathing.
Treatment depends on the location and the nature of the tumour. In cases of tumours infiltrating vitally important areas of the brain (e.g. brain stem, thalamus, mid-brain) only one sample is taken to determine the tumour type. According to the results of histopathological examination a suitable treatment method is used, in most cases radiotherapy and/or chemotherapy.
However, in most cases the primary method of treatment is surgery. Complete surgical removal of the tumour is the goal of surgical treatment. However, in cases of tumours infiltrating vitally important areas of the brain, surgery is associated with high risk of severe neurological deficits (e.g. paralysis, speech impairment). It is often safer to remove a part of the tumour. Brain tumour operations are usually performed under general anaesthesia. In the case of tumours located near the speech centre, however, it is better to perform awake brain surgery. This means that the patient is awakened after the skull is opened, so the speech can be observed during the procedure. The patient is asked to speak, read aloud, name things shown to him. It allows serious speech impairment to be avoided as a consequence of the surgery.
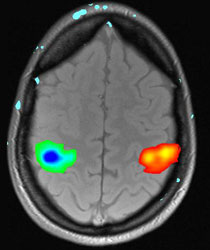
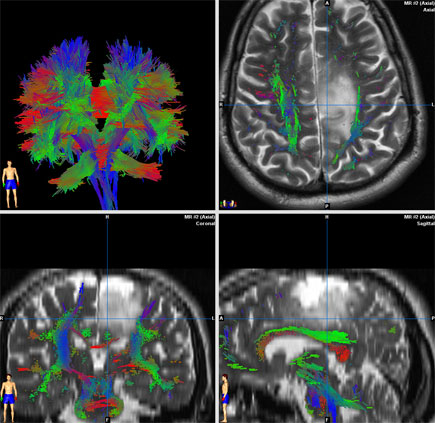
The risk of brain tumour surgery complications depends on the size and location of the tumour, as well as on its relation to the blood vessels of the brain. Age and anaesthesia related risks are also important factors. Small tumours in favourable locations can usually be operated with a rather small risk of complications. Surgery in cases of large tumours located in vitally important areas is associated with substantial risk. The risk of surgery is different in different patients, which is why individual assessment and counselling for each patient is of great importance in our clinic. Thanks to modern surgical procedures and techniques (microsurgery and endoscopy, neuronavigation with fibertracking, functional imaging, intraoperative monitoring of brain functions, intraoperative imaging) it is possible to substantially reduce the risk connected with surgical treatment. All of the aforementioned procedures and techniques are available in our clinic.
In cases of benign tumours surgery is a sufficient treatment option. Malignant tumours always require additional radiotherapy and/or chemotherapy.
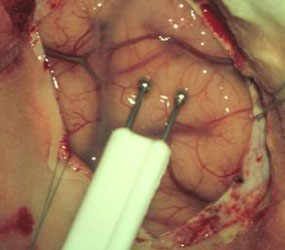
Fig 3. Intraoperative USG image
A: USG probe
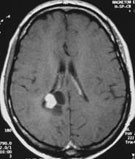
B: MRI scan of cystic brain tumours
C: USG image of the tumours