|
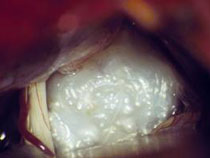
Epidermoids are tumours located at the base of the skull, in the cerebrospinal fluid space. They develop from cells that actually belong to tissues of the skin, but at the time of brain development they remained in the brain area. Epidermoids are surrounded by a thin capsule forming keratin scales. They are slowly growing tumours, showing clinical symptoms when compressing surrounding neural structures. Because of their appearance they are sometimes called “pearly tumours”. They are often located in the posterior cranial fossa and grow into all corners of the cerebrospinal fluid space. This is why the endoscopic surgical technique here offers a clear advantage. Using the endoscope the parts of the tumour not visible in the straight line view of the microscope can be located and safely removed.
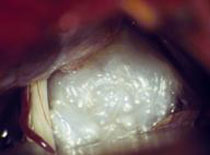
Fig. 1. Microscopic (A) and endoscopic (B, tumour under motor part of facial nerve) image of epidermoid
The symptoms can be very diverse, depending on the size of the tumour (with larger tumours causing intracranial hypertension) and its location. Brain nerves are often affected (with symptoms such as hearing loss and facial pain). Seizures are also quite common.
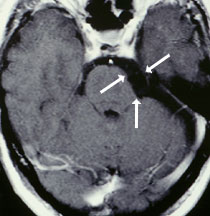
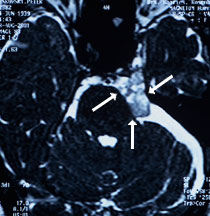
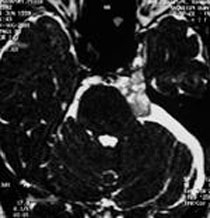
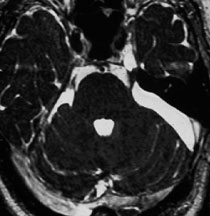
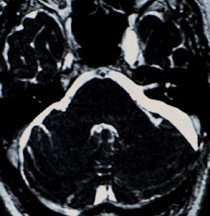
Magnetic resonance imaging (MRI) is the diagnostic method of choice. In standard MRI sequences (T1 and T2) the tumours are difficult to discern from surrounding cerebrospinal fluid. Signs of mass effect suggest presence of the tumour. CISS sequence is much more useful in finding the tumour (Fig. 2). Neurological and laryngological or ophthalmological examinations are also very important diagnostic steps necessary to assess the hearing, vision and sense of balance.
Fig. 2 MRI scan of epidermoid tumour of the cerebellopontine angle (arrow).
A: T1-weighted image showing compression of the brain stem. The tumour itself is not visible.
B: CISS sequence shows the extent of the tumour.
Complete tumour removal is the treatment of choice. Successful surgery may lead to complete recovery. Unfortunately, the tumour capsule is often connected tightly to the brain nerves or blood vessels, rendering tumour resection without causing any damage to these structures virtually impossible. In such cases it is better to leave some parts of the tumour capsule and leave the nerves or arteries intact. The growth rate of these tumours is very slow, so the recurrence risk is low. Even if a recurrence occurs, it might manifest only after many years (in one of our patients after 17 years).
Microscopic surgery with the support of an endoscope is very efficient in surgical treatment of epidermoids. Endoscopy makes it possible to remove large tumours extending over various areas of the skull using just one opening of the skull (e.g. tumours in the posterior fossa reaching the medial cranial fossa). Using just a microscope often requires several approaches from different sites of the skull.
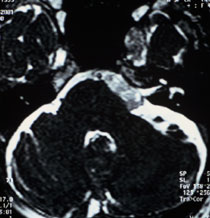
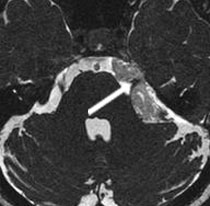
The 62-year-old patient complained of numbness in the left side of his face. MRI scans showed a small epidermoid tumour in the cerebellopontine angle with parts of it reaching the canal of the sensory facial nerve (cavum Meckeli). The tumour was removed through a small opening behind the left ear; microscopic surgery with endoscopic technique was used. Endoscopic techniques enabled removal of the tumour parts located in the canal of the sensory facial nerve. A second opening of the skull could thus be avoided. The patient recovered completely after the surgery.
Fig 3.
A and B: MRI scans (CISS sequence) showing the epidermoid tumour in the cerebellopontine angle reaching the cavum Meckeli.
C: Tumour located in cerebellopontine angle.
D: Complete removal of the tumour from the cerebellopontine angle. The part of the tumour located in the cavum Meckeli could not be seen using the microscope.
E: Removal of the tumour from the cavum Meckeli using the endoscope (30° angle).
F: Inspection of cavum Meckeli after tumour removal.
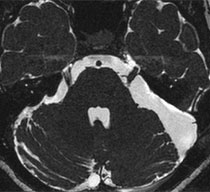
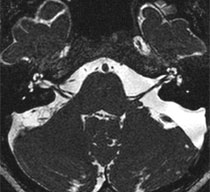
G and H: Postoperative MRI scans (2 years after the surgery) showing complete removal of the tumour.
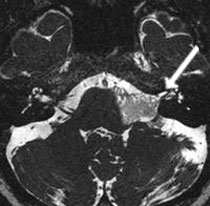
The 45-year-old female patient complained of left-sided facial pain (trigeminal neuralgia). MRI images showed a large epidermoid tumour in the cerebellopontine angle compressing and displacing sensory facial nerves. The tumour was removed through a small opening behind the left ear using microscopic surgery with the endoscopic technique. The parts of the tumour reaching the canal of the sensory facial nerves and the medial cranial fossa were removed using the endoscopic technique. A second opening of the skull could thus be avoided. All symptoms of trigeminal neuralgia resolved completely directly after the surgery.
[Translate to English:] Video 2 (3.1 MB)
Zum Starten der Videosequenz bitte auf das Bild klicken.
Fig 4.
A and B: MRI scans (CISS sequence) showing the epidermoid tumour in cerebellopontine angle displacing sensory facial nerves (arrow, Fig. A), as well as motor facial nerves and auditory nerves (arrow Fig. B).
C: Tumour growing over the sensory facial nerves (arrow).
D: Separating the tumour from the facial nerves using microscissors.
E: Removal of the tumour behind the trochlear nerve under the control of the endoscope (30° angle).
F: Microscopic image after complete tumour removal.
G and H: Postoperative MRI scans (6 months after the surgery) showing complete removal of the tumour.
|