|
In the case of acromegaly too much growth hormone is produced by the pituitary gland, usually as a result of a tumour. In adults with epiphyseal fusions it leads to slowly progressing enlargement of the extremities (nose, ears, fingers and toes). But also soft tissues (tongue, lips, as well as the inner organs/heart) increase in size. In particular the enlargement of the heart is dangerous and can lead to considerable shortening of normal life expectancy. In the case of hormone overproduction before epiphyseal fusions it leads to hypersomnia.
Fig. 1.
A: Typical enlargement of facial features in acromegaly.
B: Thickened fingers in acromegaly.
Due to insidious changes, the enlargement of ears, nose and lips is not noticed at all or noticed very late by the patient himself. Many patients report that the rings or gloves as well as shoes do not fit any more. The changes are often noticeable only to people who have not seen the affected person for a long time. However, apart from the typical enlargement of the extremities it can also lead in the case of the appropriate tumour size to disturbances of the visual field or deterioration of acuteness of vision. If additionally the other hormone axes are impaired by the tumour, there may develop signs of pituitary insufficiency with a decrease in performance, exhaustion, need for sleep and sexual disorders.
In magnetic resonance tomography one often recognizes a contrast enhancing tumour that can be limited to the pituitary gland or alternatively clearly extends beyond that.
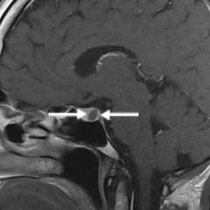
Fig. 2. MRI in acromegaly.
A: Microadenoma in acromegaly (arrows). The tumour absorbs less contrast agent compared to the normal pituitary gland.
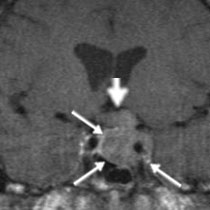
B: Invasively growing macroadenoma (arrows) with infiltration of the cavernous sinus, encircling the wall of the carotid artery (short arrow), with compression of the visual nerve (arrowhead).
The therapy of choice is surgical removal of the tumour via endonasal access. During and after the surgery the level of growth hormone in the blood is determined. If the tumour is completely removed, the hormone level immediately falls. If the level of growth hormone is below 2 µg/l, a successful cure can be assumed. The final proof of successful tumour removal with cure of acromegaly is obtained a few weeks after the surgery by hormone specialists (Privatdozent Wallaschofski, Dept. for Endocrinology, Clinic for Internal Medicine A) who can examine performance of the pituitary gland with specific hormone tests.
If cure of acromegaly is not possible by surgery alone, then either medication therapy and/or radiotherapy is carried out.
The 45-year-old man manifested typical changes in acromegaly (enlargement of nose, ears, lips, tongue, fingers and toes). During the endocrinological diagnostics a pathologically raised level of growth hormone was noted. The diagnosis of florid acromegaly was made. The subsequently arranged MRI shows a small tumour absorbing little contrast agent and located inside the pituitary gland, suggesting the presence of a growth hormone forming adenoma. The tumour was completely removed via access through the right nostril and sphenoidal sinus with the assistance of the operating microscope and endoscope. After the surgery the level of growth hormone became normalized. The postoperative MRI shows the complete removal of the adenoma with proper imaging of the normal pituitary gland. The postoperative hormone tests showed normal performance of the remaining pituitary gland, so the patient does not need any hormone substitution. The acromegaly was cured by surgery alone.
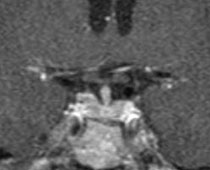
Fig. 3.
A: Typical facial expression in florid acromegaly.
B: The magnetic resonance tomography shows a small pituitary tumour inside the normal pituitary gland (microadenoma) (arrows).
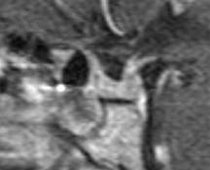
C: The postoperative MRI follow-up 1 year after the surgery shows complete tumour removal as well as a normal pituitary gland.
|