|
Hormone-inactive pituitary tumours originate in the cells of the anterior lobe of the pituitary gland. They do not deliver any hormones in the blood. Hormone-inactive pituitary tumours are usually noticeable through their space-consuming impact (pressure) on the visual nerves or the pituitary gland.
Most often the patients notice a restriction of the visual field or deterioration of vision (deterioration of acuteness of vision). However, some patients present with pituitary insufficiency (hormone deficiency). The patient then complains of exhaustion, tiredness, decrease in performance, increased need for sleep and loss of libido. The endocrinological diagnostics often show a complete or partial pituitary insufficiency of hormone axes, i.e. insufficient hormone production. Hormone overproduction as in the hormone-active tumours is not present.
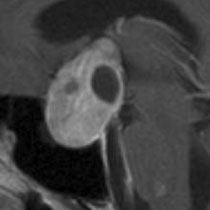
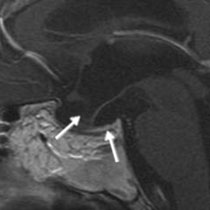
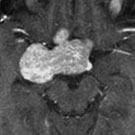
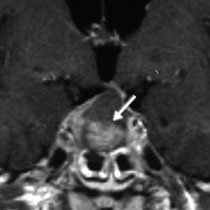
The magnetic resonance imaging often shows large tumours absorbing the contrast agent that can be solid or cystic. The optic chiasma is usually raised or displaced. In the case of pituitary apoplexy (pituitary haemorrhage) signs of acute or subacute haemorrhage in the tumour are found.
Fig. 1. A: Macroadenoma with visual nerve compression (arrows)
In hormone-inactive tumours the therapy of choice is complete tumour removal. It is achieved via endonasal (access via the nose) and sphenoid sinus access. Due to often enormous tumour size the assistance of an endoscope is very useful in order to see in every corner of the tumour cavity. Because of that the radicality of the surgery can be increased.
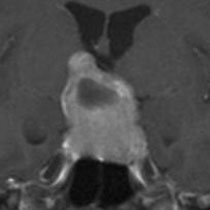
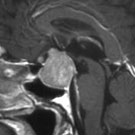
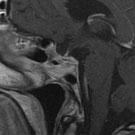
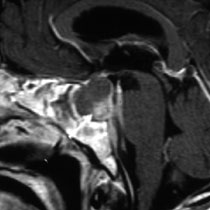
The 43-year-old patient presented with slowly progressing restriction of the visual field and deterioration of acuteness of vision, as well as headaches. The imaging diagnostics showed a large, contrast agent absorbing pituitary tumour that had stretched until well into the third ventricle. The hormone examination showed that the tumour did not secrete any hormones, but disturbed the normal hormone production (pituitary insufficiency). The tumour removal took place via the right nostril with the assistance of a microscope and in particular an endoscope. The tumour could be completely removed. The postoperative MRI follow-up showed complete tumour removal, as well as the preserved, clearly atrophied residual pituitary gland (see Fig. 2 c). After the surgery the patient is free of complaints and the visual disorders resolved well, but he continues to require pituitary hormone replacement therapy since due to the tumour size only a little normal pituitary tissue is left.
Fig. 2.
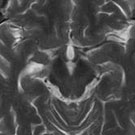
A: The magnetic resonance imaging shows a large, contrast agent absorbing pituitary tumour that considerably extended beyond the bony encasement of the pituitary gland and into the cerebral tissue.
B: The video shows the complete tumour removal.
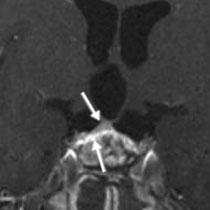
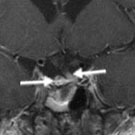
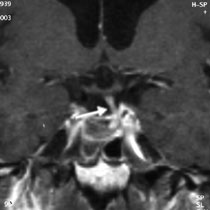
C: The postoperative MRI follow-up 6 months after the surgery shows the complete tumour removal, as well as the preserved pituitary stalk (long arrow) and the preserved thin normal pituitary tissue (short arrow). The sphenoidal sinus was filled with adipose tissue in order to prevent postoperative cerebrospinal fluid fistula.
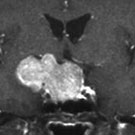
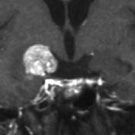
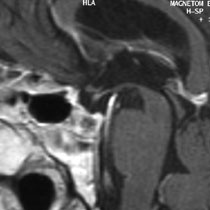
The 56-year-old patient presented with impaired vision with restriction of the visual field and signs of pituitary insufficiency. The imaging diagnostics showed a large pituitary tumour that extended not only in the centre line upwards, but also spread to the right side in the temporal lobes (Fig. 3 A). The endocrinological diagnostics showed that the tumour did not produce any hormones. However, normal hormone production was already considerably restricted. The tumour was resected at first via endonasal access (through the nose) (Fig. 3 B). The tumour tissue that was in the centre line could be completely removed inside the pituitary gland region as well as above it. The postoperative MRI follow-up shows complete tumour removal in the region of the centre line (Fig. 3 C). The tumour part located on the right, next to the pituitary gland region, could not be removed from that access. Therefore, 2 months after the surgery a second operation took place via a right eyebrow incision. During this surgery the tumour that had developed below the right optic nerve and round the right cerebral artery could be completely removed (Fig. 3 D). The postoperative MRI follow-up shows complete tumour removal as well as the preserved pituitary stalk with the adjoining narrow normal pituitary tissue (Fig. 3 E). The visual disorders had considerably improved already after the first surgery. The endocrinological diagnostics showed that hormone replacement is necessary. The cosmetic result 6 months after the eyebrow incision was excellent – the scar was hardly visible (Fig. 3 F).
Fig. 3.
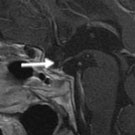
A: MRI with imaging of the large contrast agent absorbing pituitary tumour that had developed on the right side, next to the pituitary gland region.
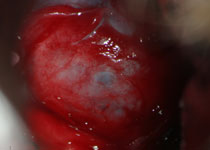
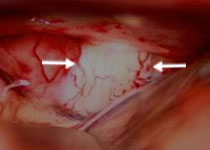
B: Endoscopic imaging shows tumour removal with the assistance of vacuum and curette. Visible are typical whitish deliquescent pituitary tissue.
C: The postoperative MRI 2 months after the first surgery shows complete tumour removal in the region of the centre line, as well as the residue of tumour on the right, next to the pituitary region.
D: Microscopic imaging shows the optic nerve (arrows), as well as the underlying yellowish tumour. The tumour is completely removed under microscopic and endoscopic visual control.
E: The postoperative MRI follow-up 6 months after the second surgery shows complete tumour removal with the residual edge of the pituitary gland.
F: The photo shows the patient 6 months after the surgery. An excellent cosmetic result can be seen, with a barely visible scar in the region of the right eyebrow.
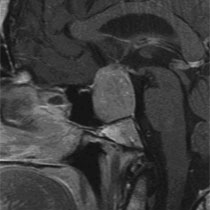
Pituitary apoplexy
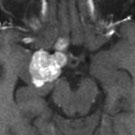
A 64-year-old patient had a pituitary tumour treated with Pravidel. Three months later the patient suddenly complained of acute headaches. Four days later an acute deterioration of vision with restriction of the visual field, decline of acuteness of vision and paralysis of the right oculomotor nerve (ptosis and pupil enlargement) occurred. The immediately carried out magnetic resonance imaging showed a pituitary adenoma with acute haemorrhage (see arrow). The video shows the tumour removal under endoscopic visual control. After the incision of the tumour capsule a black, motor oil-like blood empties that is indicative of a subacute haemorrhage. It can be clearly seen how one can radically remove the tumour under direct visual control with the endoscope in the corners between the meningeal lining of the region of the pituitary gland and the adjoining venous cavernous sinus (corner between the cavernous sinus and dura or sellar diaphragm). The postoperative MRI shows complete tumour removal with a preserved pituitary stalk. The visual disorders fortunately resoled quickly. Further hormone replacement is necessary since the tumour caused major damage to the pituitary gland.
Fig. 4.
A: Large pituitary adenoma with acute haemorrhage (see arrows)
B: The video shows the endoscopic surgical technique with complete tumour removal under endoscopic visual control.
C: The postoperative MRI 1 year after the surgery shows complete tumour removal with a preserved pituitary stalk (see arrow).
|