|
Colloid cysts are benign cystic structures that typically occur in the anterior upper region of the third ventricle. If they displace the crossing from the lateral ventricle to the third ventricle (foramen of Monro), an impediment to passage of cerebrospinal fluid occurs and consequently hydrocephalus.
Colloid cysts usually manifest in adulthood through clinical symptoms such as headaches, nausea, vomiting, disturbances of equilibrium or restrictions of concentration and memory. In some patients presented to us the cyst was discovered as incidental finding. However, colloid cysts can also lead to an acute increase of cerebral compression with coma and lethal consequences due to rapidly developing hydrocephalus, and because of that they require particular attention.
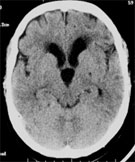
Computed tomography (CT) can show a colloid cyst as a hyperdense or hypodense lesion at the vault of the third ventricle. Additionally, the CT can show the signs of hydrocephalus with extension of the lateral ventricle.
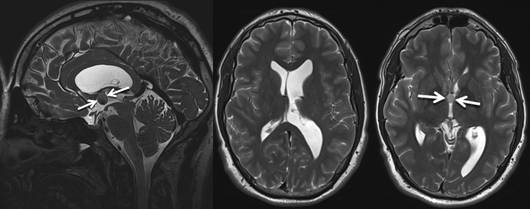
In order to enable the detailed presentation of a colloid cyst, magnetic resonance imaging (MRI) is considered necessary. In particular, imaging on three levels is relevant when deciding about the therapy as well as when planning the surgery.
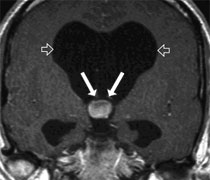
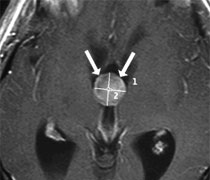
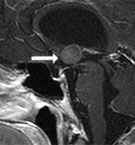
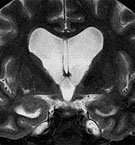
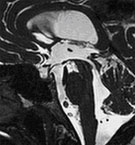
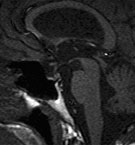
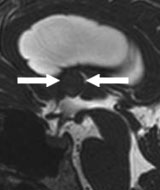
Fig. 2. Magnetic resonance imaging of a colloid cyst in the third ventricle (arrows) in coronary, axial and sagittal sectional plane. One can see the beginning of disturbance of cerebrospinal fluid circulation with development of hydrocephalus (open arrows).
Colloid cysts that do not disturb the cerebrospinal fluid circulation should be monitored at regular intervals by cerebral imaging (CT or preferably MRI) with reference to the size and form. Cysts that are symptomatic due to hydrocephalus should be operated on as soon as possible. Since colloid cysts can lead to an acute increase of cerebral compression with coma and lethal consequences due to rapidly developing hydrocephalus, we usually recommend cyst removal, including in the case of asymptomatic cysts that have already led to disturbance of cerebrospinal fluid circulation. Multiple case reports about the sudden loss of consciousness in patients with previously undiscovered colloid cysts indicate that preventive surgery is reasonable.
In principle, there are two methods of surgery. Colloid cysts can be removed microsurgically by a craniotomy (skull opening). This therapy was considered to be a standard procedure and usually permitted complete cyst resection. We favour in our clinic a minimally invasive endoscopic procedure with which the majority of cysts can be completely removed.
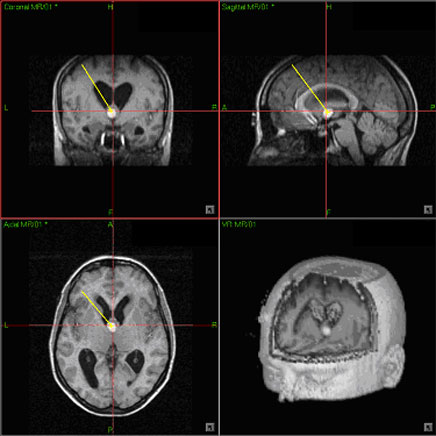
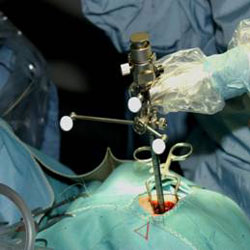
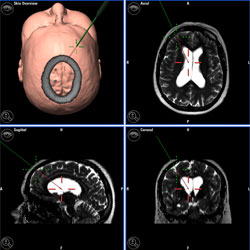
In order to reach the cyst optimally, the position of the access point for the endoscope is planned with neuronavigation (Fig. 3). After inserting the endoscope in the front part of the lateral ventricle (anterior horn of lateral ventricle) the colloid cyst can be removed under endoscopic visual control with special instruments (endoscopic scissors, tenaculum forceps, coagulation electrodes, suction catheter). The present literature shows that the long-term results of endoscopic surgery concerning success rate, tendency to recurrence and complications favour the microsurgical operation. The advantage of the endoscopic method is that by the endoscopic access less cerebral tissue is damaged than in open surgery (diameter of the endoscope 6.8 mm). The patients can be very quickly completely mobilized after the surgery.
In the aftercare regular MRI follow-ups are of high significance. Even though in our clinic no recurrence of a colloid cyst has been seen yet after endoscopic surgery, cases of recurrences after more than ten years are described in the neurosurgical literature. That is why long-term follow-up with regular MRI imaging is necessary.
The 59-year-old female patient complained of headaches, disturbances of memory and powers of concentration, as well as disturbances of equilibrium. In the CT a colloid cyst can be seen in the third ventricle. The cyst was endoscopically completely removed under neuronavigation. The headaches and disturbances of equilibrium resolved.
Fig. 4.
A: The computed tomography shows a colloid cyst (arrow) with a blockage of the foramen of Monro.
B: Neuronavigation for access planning.
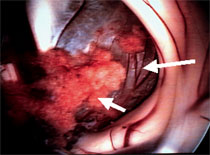
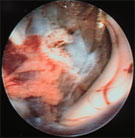
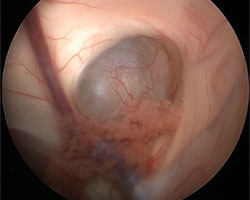
C: The video shows endoscopic cyst removal. At first coagulation of the cyst wall. Afterwards opening of the cyst with scissors, aspiration of the cyst contents and removal of the cyst membrane.
D: The postoperative computed tomography shows complete cyst removal.
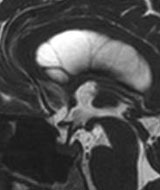
The 37-year-old patient presented with headaches, general tiredness, exhaustion and a drop in performance. The magnetic resonance imaging (MRI) showed a large colloid cyst in the third ventricle and an enormous extension of the ventricles. The cyst was endoscopically completely removed. After the surgery the symptoms resolved completely within a few weeks. The MRI done 2 years after the surgery shows complete cyst resection and a clear reduction of the extent of the ventricles with free passage of cerebrospinal fluid.
Fig. 5.
A: The MRI shows a large colloid cyst (arrow) at the vault of the third ventricle that had led to occlusion hydrocephalus with enormous extension of lateral ventricles.
B: The cyst membrane after complete removal from the ventricle.
C: The MRI 2 years after the surgery shows complete cyst removal and reduced extent of the ventricles.
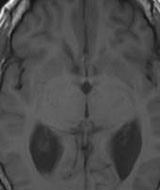
The 42-year-old female patient presented with a character change and complained of headaches. The MRI showed a colloid cyst in the third ventricle that led to retention of cerebrospinal fluid (ventricles clearly extended). The cyst was endoscopically completely removed under neuronavigational control. The symptoms resolved completely.
Fig. 6
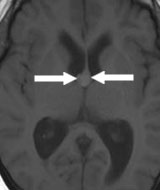
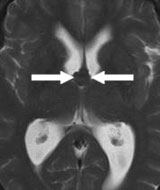
A-C: The MRI images show the colloid cyst in the third ventricle (A = T1 sequence axial, B = T2 sequence axial, C = CISS sequence sagittal).
D: Endoscope shaft with navigation adapter.
E: Navigational access planning.
F: Video of the cyst removal.
G – I: Postoperative MRI images show complete cyst removal.
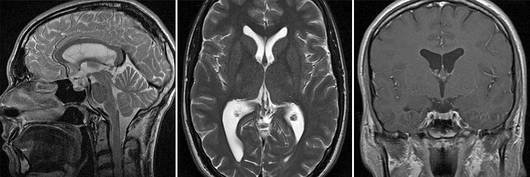
The 22-year-old male student presented with increasing headache, pressure feeling in the head, and vomiting. MR imaging showed a colloid cyst (arrows) with obstruction of both foramina of Monro and dilation of both lateral ventricles.
MR imaging obtained two years after surgery confirms the absence of any cyst remnant. The ventricles decreased markedly in size. The patient is free of symptoms.
|