Gliomas constitute ca. 40% of brain tumours. The most common type of glioma is glioblastoma (50%), followed by astrocytoma (ca. 30%), oligodendroglioma (ca. 8%) and ependymoma (ca. 6%). There are also mixed gliomas, such as oligoastrocytoma and glioneural tumours (e.g. ganglioglioma). The tumours are classified according to their biological properties. In WHO classification systems the tumours are graded from grade 1 (benign, clearly delineated from surrounding tissues) to grade 4 (highly malignant tumours). Tumours graded 2, 3 and 4 infiltrate surrounding tissues, which leads to high recurrence rates, even after seemingly complete removal of the tumour.
Diagnosis includes complete physical examinations and imaging techniques. MRI is the diagnostic method of choice. Additional tests (such as CT scans, MRI of spinal column, ophthalmological or laryngological examination, CSF examination, angiography, blood tests, electrophysiological examination) are in most cases not necessary.
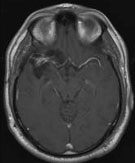
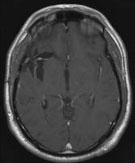
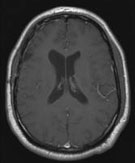
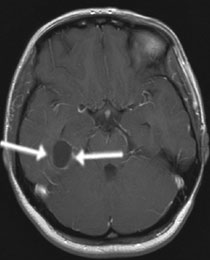
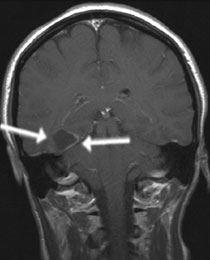
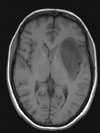
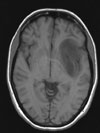
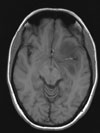
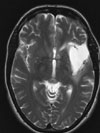
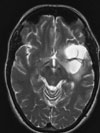
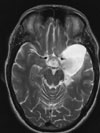
Fig 1: MRI scans of brain tumours (arrow)
A: Oligodendroglioma B: Glioblastoma C: Subependymoma
In most cases of glioma surgery is the first-line therapeutic option. In patients with grade 1 tumours (WHO) surgery can lead to complete recovery. If complete removal cannot be achieved, regular MRI check-ups are required to assess the growth rate of the tumour. If remaining tumour fragments do exhibit a tendency to grow back, repeated surgery or adjuvant therapies (radiotherapy and/or chemotherapy) can be considered. Malignant gliomas (WHO grade 3 and 4) always require postoperative radiotherapy and/or chemotherapy, even if MRI scans suggest complete removal of the tumour mass. In case of inoperable tumours tissue samples of the tumour are taken to determine its type and plan suitable treatment.
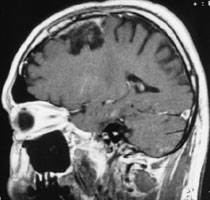
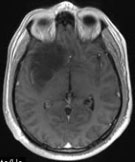
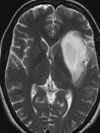
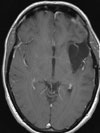
Glioblastoma is a very malignant type of brain tumour. It affects mostly patients over 50 years old. Symptoms include mostly signs of intracranial hypertension, seizures and neurological deficits, such as visual impairment, and paralysis. MRI scans show contrast enhancing tumours, with necrotic areas and swelling of the surrounding tissues. Surgery is in most cases followed by a combination of radiotherapy and chemotherapy, which means that chemotherapy is applied in parallel to radiotherapy. Recurrence rates are very high, but there are isolated cases of patients remaining symptom-free years after the treatment.
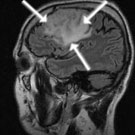
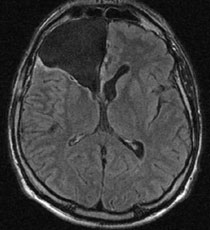
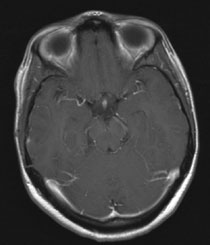
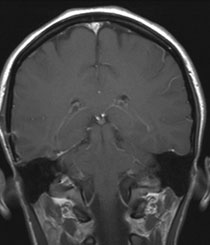
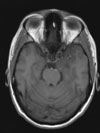
Fig 2.
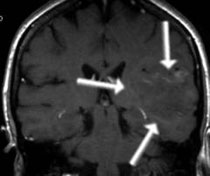
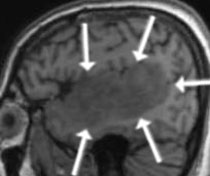
A: MRI scans taken from a 42-year-old patient with a large glioblastoma in the right frontal horn (arrow). The patient complained at first of headache.
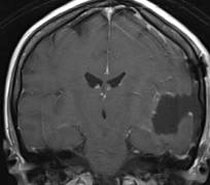
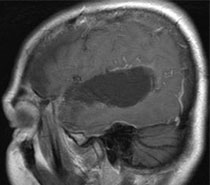
B: MRI scans taken 4 years after the surgery and radiotherapy showing the post-resection cavity with no sign of recurrence. The patient displayed no neurological deficits and could take up his former job working full-time.
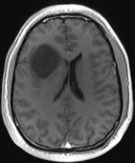
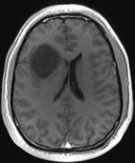
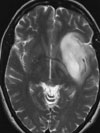
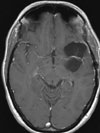
Pilocytic astrocytomas (WHO grade 1) occur mostly in children and adolescents (see brain tumours in children). Astrocytomas grade 2 and 3 occur mostly in adults. Seizures are often the first manifestation of astrocytoma. In MRI scans they can present as either sharply delineated or diffuse infiltrating surrounding tissues. Grade 2 tumours typically do not take up contrast agent, in contrast to grade 3. Surgery is in most cases the first choice treatment. However, the extent of resection is mostly limited due to the infiltration of vitally important brain areas. Astrocytomas of grade 2 tend to gain in malignancy with ca. 60% of cases passing from grade 2 to grades 3 and 4. Recurrences are common.
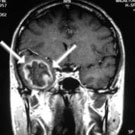
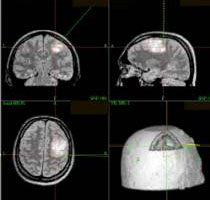
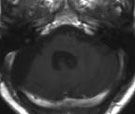
Fig 3.
A: MRI of a 47-year-old patient with grade 2 astrocytoma (arrow). The first clinical symptom was a seizure attack.
B: Image of the neuronavigation. The tumour infiltrated the motor area responsible for arm and leg muscles; complete removal of the tumour was not possible.
C: Postoperative MRI scans show the results 3 years after the surgery with no tendency to grow back. With the exception of slight impairment of left hand mobility, the patient displayed no other neurological deficits.
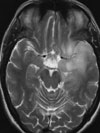
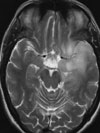
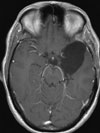
Oligodendrogliomas manifest themselves commonly through seizures. MRI scans show tumours sharply delineated from the brain tissues. Grade 2 tumours, in contrast to grade 3, do not take up contrast agents. Calcifications are often observed. Surgery is the first-line treatment. However, the extent of resection is mostly limited due to the infiltration of vitally important brain areas. The remaining tumour fragments however can remain for years with no tendency to grow back. The prognosis in oligodendrogliomas is more favourable than in astrocytomas. Gaining in malignancy is rare. Recurrences occur later. In the case of large, inoperable tumours, chemotherapy can often be surprisingly successful.
[Translate to English:] Video 1 (3.1 MB)
Zum Starten der Videosequenz bitte auf das Bild klicken.
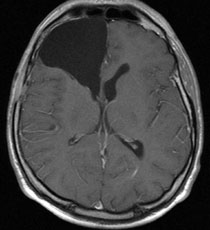
Fig 4.
A: MRI of a 34-year-old patient with oligodendroglioma in the right insular area. The first clinical manifestation was a seizure attack.
B: The video shows removal of the tumour growing around the middle brain artery.
C: MRI scan taken 1 year after the surgery, showing the resection cavity with no signs of recurrence. The patient displayed no neurological deficits and returned to his previous job as a full-time chef.
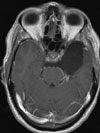
Ependymomas arise from the lining of the ventricles of the brain and spinal tap (ependyma). Due to their location they often lead to accumulation of cerebrospinal fluid. Surgery is the first-line treatment option. Ependymomas are in most cases relatively easy to separate from the healthy brain tissues, which is helpful for the surgeons. Only in the case of malignant tumours or inoperable remains of the tumours can radiotherapy be used.
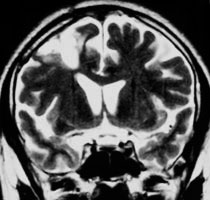
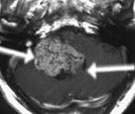
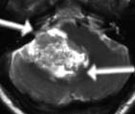
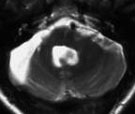
Fig 5.
A: MRI imaging of a 56-year-old male patient with a large ependymoma in the fourth brain ventricle and cerebellopontine angle (arrow). The first clinical symptoms in this patient included impairment of the sense of balance and vomiting.
B: MRI scan taken 5 years after the surgery, showing no signs of recurrence. Apart from slight hoarseness the patient was symptom-free.
Gangliogliomas are mixed tumours (mostly WHO grade 2) containing elements of glial cells (forming the tissue “supporting” the brain) and neural cells. They grow rather slowly and can be easily separated from the healthy brain tissue. Surgery is the first-line treatment option. Only in the case of malignant tumours (grade 3 and 4) is radiotherapy and/or chemotherapy used.
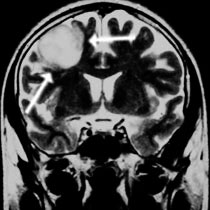
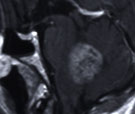
Fig 6.
A: MRI of a 17-year-old girl with ganglioglioma in the right temporal area of the brain (arrow). First clinical symptoms were visual deficits.
B: Small skull opening (mini craniotomy) over the base of the skull.
C: The bony lid being put back in place, fixed with titanium clips.
D: MRI scan taken 2 years after the surgery showing complete tumour removal. The patient displays no neurological deficit.
Insular gliomas belong to the most challenging brain tumours as far as surgical techniques are concerned. They are situated in the vicinity of important brain structures (motor pathways, visual pathways, speech centre, basal ganglia) and blood vessels, which results in high operational risk. Careful monitoring during the surgery is required in order to avoid neurological deficits. Since the speech centre is mostly located in the left hemisphere, left-sided tumours are removed in our clinic during awake brain surgery.
Video 2 (0.7 MB)
Click to start the video.
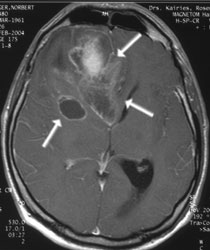
Fig 7.
A: MRI scan of a 45-year-old female patient with a large, left-side astrocytoma in the insular area (arrow) and left temporal lobe. First clinical symptoms in that patient included speech disturbances and seizure.
B: The tumour was resected during awake brain surgery. Complete removal was not possible, since the tumour infiltrated the sensory speech centre and visual pathway. Nevertheless, a large portion of the tumour could be removed. Monitoring of speech during the operation allowed safe assessment of the percentage of the tumour to be removed.
C: MRI scan 2 years after the surgery, showing a vast resection cavity, with no signs of recurrence of remaining tumour tissue. The patient displayed mild memory disturbances, with no other neurological deficits.
Fig 8.
A: MRI of a 39-year-old female patient with a large oligoastrocytoma in the left insular region. First clinical manifestation was a seizure.
B: Functional MRI showing left sided speech centre localisation. The tumour borders directly with the motor speech centre (red field).
C: The tumour was resected during awake brain surgery to monitor speech and motor functions (movements of the right extremities). The distal part of the tumour could not be removed, since visual pathways would be damaged.
D: MRI scan 1 year after the surgery showing a vast resection cavity with no sign of recurrence. The patient displays no signs of neurological deficit, with some neuropsychological deficits that had been expected prior to the surgery (she is undergoing intensive cognitive training to compensate for this problem).
Contact:
Dr. med. St. Fleck, Tel.: 03834-86-6163, Fax: 03834-86-6164, E-Mail: fleck@uni-greifswald.de
or
Prof. Dr. med. Henry W. S. Schroeder, Tel.: 03834-86-6162, Fax: 03834-86-6164,
E-Mail: Henry.Schroeder@uni-greifswald.de
|