|
Craniopharyngiomas are benign malformation tumours that develop from the remnants of Rathke’s pouch and usually originate in the pituitary stalk. They grow slowly and are symptomatic through compression of the nerve structures. They often cause the retention of cerebrospinal fluid with development of hydrocephalus due to expansion in the third ventricle.
Fig. 1. Microscopic and endoscopic image of craniopharyngioma.
Craniopharyngiomas often cause vision disorders by compression of visual nerves. If the tumour is not treated and it progresses, there is a danger of blindness. Furthermore, the tumours are often noticeable by disturbances of hormonal regulation. Due to insufficient hormone production the patients complaint of a decrease in performance, exhaustion, increased need for sleep, thirst, impotence and loss of libido. The lack of hormones can have consequences ranging from disturbances of consciousness to coma. Furthermore, mental symptoms with disturbances of memory, character change and disorientation are possible. The retention of cerebrospinal fluid can lead to symptoms of cerebral compression with headaches, nausea and vomiting.
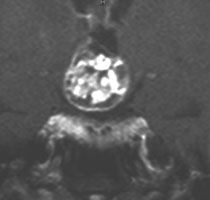
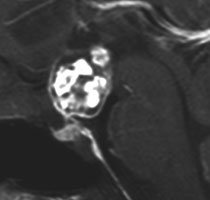
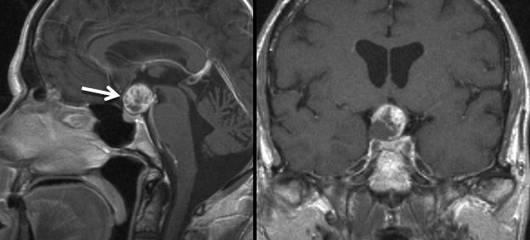
Magnetic resonance imaging (MRI) is the examination of choice. Craniopharyngiomas are located in the region of the pituitary gland (hypophysis), pituitary stalk or in the third ventricle. They are usually cystic, absorb contrast agent or have a solid part absorbing contrast agent. Calcifications are frequent (Fig. 2).
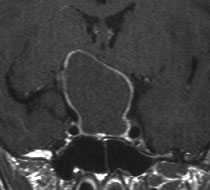
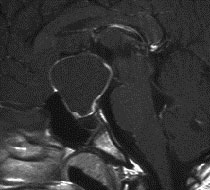
Fig. 2 The magnetic resonance image of a large cystic craniopharyngioma with visual nerve compression.
There has been a lot of discussion about the best form of treatment of craniopharyngiomas in the specialist literature. There are no major studies that resolve the issue incontrovertibly. From our point of view the therapy of choice is complete tumour removal. Because of the surgery a cure is possible, even though recurrences after complete removal can occur. Since it is a benign tumour, partial tumour removal with subsequent radiotherapy is the therapy of second choice. The long-term effects of radiotherapy are not trivial. The risk of major operation lies in impairment of interbrain function with disturbances of regulation of the inner environment of the body up to coma. Crucial here is the infiltration of the interbrain (hypothalamus) by the tumour. Usually during surgery the glial zone is present round the tumour that enables complete tumour removal without these disturbances. Whether the tumour is demarcated from the brain becomes apparent only during surgery and cannot be determined before surgery. The pituitary stalk is usually not functionally maintainable (only possible in the case of small tumours), so the pituitary hormones have to be replaced after surgery.
In operations on craniopharyngiomas endoscopic-assisted microsurgical technique is well established. Using the endoscope, poorly accessible areas under the optic chiasma and in the third ventricle can be inspected.
A 37-year-old patient presented with exhaustion, decrease in performance and erectile dysfunction. The MRI showed a suprasellar craniopharyngioma with an ingrowth in the third ventricle. The endocrinological examination showed a partial insufficiency of pituitary gland function. The tumour was removed via frontotemporal craniotomy under microscopic and endoscopic visual control. The video shows the removal of the tumour between the visual nerves. Tumour parts in the third ventricle were removed under endoscopic visual control. The patient after surgery has been neurologically inconspicuous. Due to insufficiency of the pituitary gland, the hormones have to be replaced.
Fig. 3.
A and B: T1-weighted sagittal and coronary MRI images with contrast agent show suprasellar and intraventricular craniopharyngioma (bitemporal hemianopsia).
C: Tumour resection through lamina terminalis under microscopic visual control.
D: Removal of intraventricular remaining tumour under endoscopic visual control.
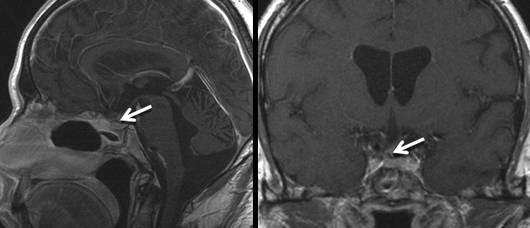
E and F: T1-weighted MRI images with contrast agent 3 years after surgery show complete tumour removal.
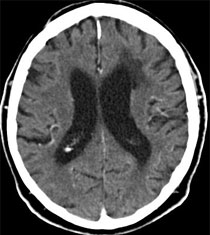
A 72-year-old patient presented with slowly progressing dementia. On admittance to our clinic he was already very sleepy (transition to coma). The CT showed a large cystic craniopharyngioma with retention of cerebrospinal fluid (occlusive hydrocephalus). The tumour was endoscopically resected via a small borehole so the cerebrospinal fluid drainage was free again. The patient recovered very well after surgery. Neurological findings are minimal. The disturbances of memory resolved well. The function of the pituitary gland is proper so no hormone replacement is necessary.
Video 2 (3.4 MB)
Click to start the video.
Fig. 4.
A and B: The CT images show ventricular system intensively expanded by a cystic tumour (arrow) in the third ventricle.
C: Cyst wall of tumour in the third ventricle.
D: Solid tumour part during endoscopic resection.
E and F: Postoperative CT shows normalization of ventricular width and tumour resection.
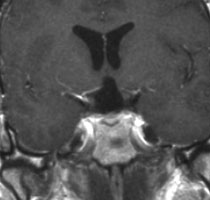
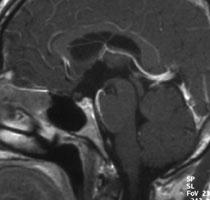
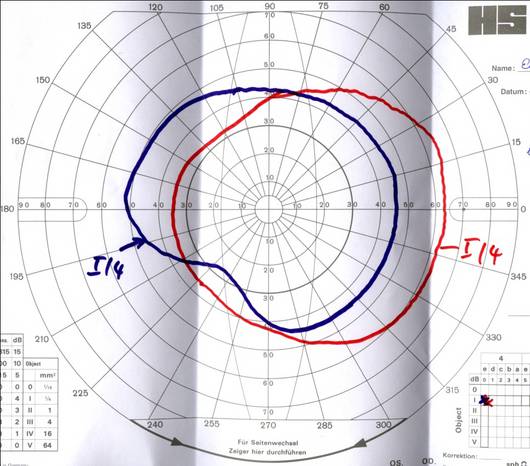
This 57-year-old male presented with severe visual impairment and a narrowed visual field. The ophthalmologic examination recorded visual acuity of 0.1 in the left eye and 0.2 in the right eye as well as severe bitemporal hemianopsia. MR imaging identified the cause of the symptoms as an inhomogeneously enhancing, suprasellar lesion with compression of the optic chiasm and prefixed chiasm. According to MRI criteria, a craniopharyngioma was suspected.
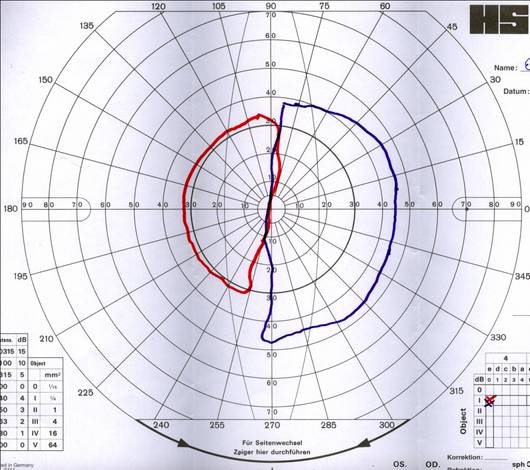
The ophthalmologic deficiencies improved quickly following the operation. Measurement of the visual field 14 days postoperatively already showed a considerable improvement of the outer limits. One year after the operation, the visual field is now only slightly narrowed in the lower quadrant. Visual acuity is 1.0 in the right eye and 0.9 in the left eye. The diabetes insipidus which developed shortly after the operation has also completely disappeared. Due to partial insufficiency of the gonadotropic and thyreotropic axes, the patient has to continue taking testosterone and thyroxine supplements. The adrenocorticotropic axis is intact. MR imaging one year after the operation showed complete removal of the tumor with a preserved pituitary stalk and pituitary gland. Two years after surgery, no recurrence has occurred.
|