|
Tumours of the peripheral nerves are usually benign schwannomas, also referred to as neurinomas or neurofibromas. They originate in the Schwann cells of the nerve sheath. Malignant tumours of the peripheral nerve sheath occur rarely.
The typical feature is a sturdy swelling in the course of a nerve. When percussing the swelling electrical paraesthesia occurs. Also paralyses of the nerve can occur later. In the case of malignant tumours rapidly progressing neurological failures (paralyses, sensory disturbances) occur.
The diagnostic process includes a clinical examination and subsequently magnetic resonance imaging (MRI) of the corresponding region.
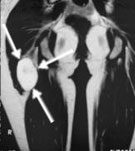
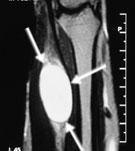
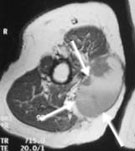
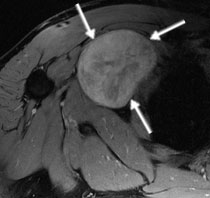
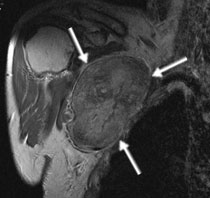
Fig. 1: MRI images of nerve tumours (arrows)
A: Neurofibroma of the sciatic nerve
B: Schwannoma of the median nerve
C: Malignant peripheral tumour of the nerve sheath of the median nerve
Microsurgical tumour removal is the therapy of choice. In the case of benign schwannomas the nerve function can usually be almost completely preserved through a careful dissection technique. Only the nerve fibre that is the source of the tumour is cut. All other nerve fibres are preserved. Recurrences are extremely rare. In the case of malignant peripheral tumours of the nerve sheath complete tumour removal along with surrounding normal tissue is the only chance of a cure. If necessary, amputations are also performed. Radiotherapy and chemotherapy are carried out in inoperable tumours but are not very effective. These tumours also form metastases in other organs. Generally, the prognosis for malignant peripheral tumours of the nerve sheath currently remains poor.
The most common extradural tumours are metastases of other tumours (80%). Lung cancer, breast cancer, renal cancer and prostate cancer particularly often cause vertebral metastases. But also plasmacytomas, lymphomas, sarcomas, osteomata, chordomas and chondromas can be found in the spine. Tumours of vertebral bodies can lead to instability of the spine. Spontaneous fractures without a causative trauma are common. Due to a fracture or space-consuming lesion there can be transverse symptoms. The aim of the surgery is decompression of the spinal cord or nerve roots, as well as stabilization of the spine. After the surgery usually radiotherapy is carried out.
Fig. 2.
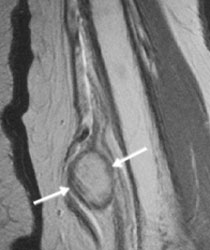
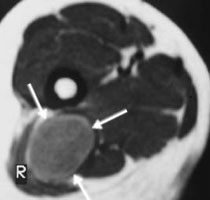
A: MRI of an 80-year-old female patient with schwannoma of the median nerve in the upper arm (arrows). The patient complained of electrical paraesthesia.
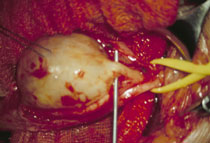
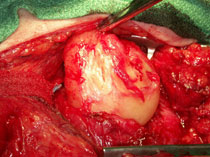
B: Tumourous distention of the median nerve.
C: Image of the nerve fibre that is the source of the tumour, above the tumour.
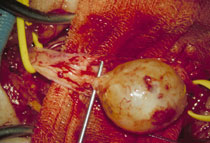
D: Image of the nerve fibre that is the source of the tumour, below the tumour.
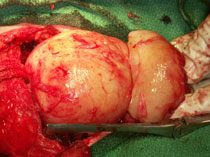
E: Unimpaired median nerve after removal of the tumour.
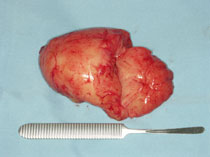
F: Tumour. The patient is free of complaints and neurologically normal.
Fig. 3.
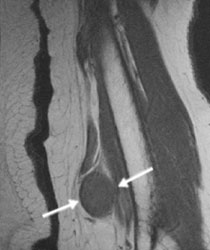
A: MRI of a 29-year-old female patient with neurofibroma of the sciatic nerve in the upper leg (arrows). The patient complained of electrical paraesthesia in the leg.
B: On the exposed tumour the intact nerve fibres can be seen.
C: Image of the nerve fibre that is the source of the tumour.
D: Separating the tumour from the nerve.
E: Tumour. The patient is free of complaints and apart from mild numbness at the back of the upper leg neurologically normal.
Fig. 4.
A: MRI of a 55-year-old male patient with neurofibroma of the brachial plexus (arrows). The patient complained of electrical paraesthesia in the right arm and weakness of the hand musculature.
B: Tumour under the nerves encircled with yellow areas.
C: Removal of nerve fibres from the tumour.
D: Mobilization of the tumour.
E: Tumour. The patient is free of complaints and neurological deficiencies.
|