|
Spinal tumours are growths of the spine. They can start from the vertebrae (extradural tumours) or lie inside the meninges (intradural tumours). Among the intradural tumours can be distinguished spinal cord tumours (intramedullary tumours) and extramedullary tumours that do not originate in the spinal cord. If untreated, they almost always lead to pressure damage of the spinal cord and due to that eventually to paraplegia.
The most common symptoms of spinal tumours is pain and neurological disturbances, e.g. numbness, weakness, bladder and rectal disorders and disorders of sexual functions. The scale of the afflictions depends on the tumour location: tumours in the middle thoracic spine can lead to paralysis of the legs; tumours in the cervical spine region can lead to paralysis of the arms and legs. Because the tumours often grow very slowly, the symptoms develop insidiously and are initially hardly noticed by the patient. Sometimes the progressively insecure gate is noticed first by relatives.
The diagnostic process involves clinical examination and subsequently imaging examination. Due to having the highest resolution for soft tissue, magnetic resonance imaging (MRI) is the method of choice in order to assess the compression of the spinal cord or the nerve fibres. To assess the stability of the spine computed tomography (CT) is carried out.
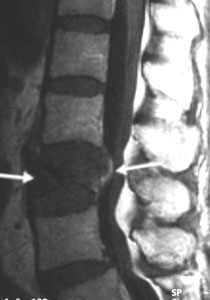
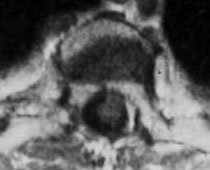
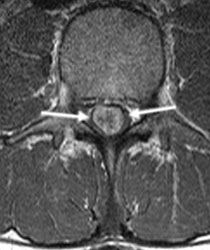
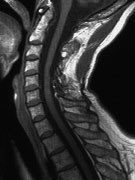
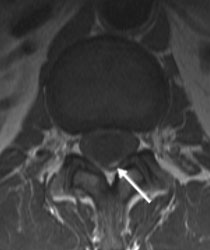
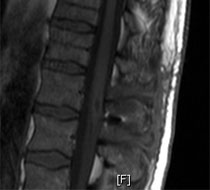
Fig. 1: MRI images of spinal tumours (arrows)
A: Vertebral body metastasis of a renal carcinoma at the level of the third thoracic vertebra with substantial compression on the spinal cord.
B: Intradural ependymoma
C: Extensive intramedullary ependymoma C5 - T4
In most spinal tumours the therapy of choice is surgery. The surgery is to relieve the spinal cord or nerve roots and/or to stabilize the spine. If it is a benign tumour, the cure can be aimed at after the complete tumour removal. In the case of malignant tumours, e.g. metastases, radiotherapy and/or chemotherapy takes always place after the surgery. If the patient has paraplegia, intensive rehabilitation therapy in the paraplegic department of the neighbouring Greifswald neurological rehabilitation centre takes place after the acute treatment.
The most common extradural tumours are metastases of other tumours (80%). Lung cancer, breast cancer, renal cancer and prostate cancer are often particularly responsible for spinal metastases. However, also plasmacytomas, lymphomas, sarcomas, osteomas, chordomas and chondromas can be found in the spine. Tumours of the vertebral bodies an lead to spine instability. Spontaneous fractures without causative trauma are frequent. Because of a fracture or space-consuming lesion it can lead to transverse symptoms. The aim of the surgery is decompression of the spinal cord or nerve roots as well as stabilization of the spine. After the surgery usually radiotherapy takes place.
Fig. 2. 56-year-old patient with metastatic renal cell carcinoma of the fourth vertebral body. The patient complained of strong neck pain and tingling sensation in the legs.
A: The X-ray imaging shows destruction of the cervical vertebra (arrows).
B: The MRI shows spinal cord compression (arrow).
C: A resection of the destroyed cervical vertebra and the subsequent reconstruction of the cervical vertebral body with a titanium basket took place. The titanium basket is fixed with a bolt and plate system. C: The postoperative X-ray imaging shows the correct position of the implant and the physiological position of the spine.
D: The postoperative MRI shows the relief of the spinal cord. The patient was free of complaints without neurological failures.
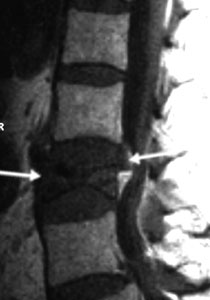
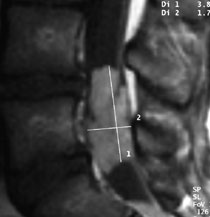
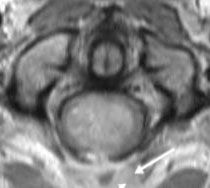
Fig. 3: A 67-year-old patient with metastatic renal cell carcinoma of the third lumbar vertebral body. The patient complained of severe pain in the back and numbness in the legs.
A: In the MRI one can see destruction of the cervical vertebra and compression of the nerve roots (arrows).
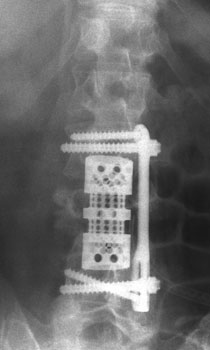
B: A resection of the destroyed lumbar vertebral body and the subsequent reconstruction of the cervical vertebral body with a titanium implant. The spine substitute was fixed with the bolt and plate system.
C: The postoperative X-ray images show the correct position of the implant and the physiological position of the lumbar spine. The patient was almost free of complaints and without neurological failures.
The most common intradural tumours are meningiomas (tumours of the meninges) and neurinomas (tumours of the nerve roots). But also ependymomas and lipomas occur. Since these tumours are almost always benign, complete tumour removal is the aim of the surgery. Radiotherapy is not useful.
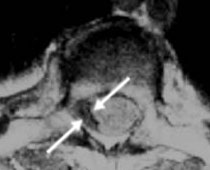
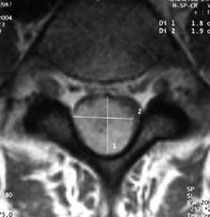
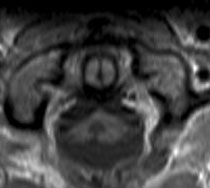
Fig. 4. A 67-year-old female patient with intraspinal meningioma at the level T 1/2. The patient complained of paraesthesia in both legs and slowly progressing insecure gate.
A: The MRI shows the contrast enhancing tumour (arrows) that almost completely depleted the spinal cord canal.
B: The grey sickle-shaped structure (between the arrows) at the edge of the spinal cord canal is the remaining spinal cord.
C and D: The postoperative MRI images show complete tumour removal with good relief of the spinal cord. Due to the long-term duration of afflictions, the sensory disturbances resolved only partly. The postural control has become more secure.
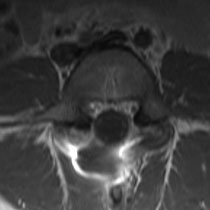
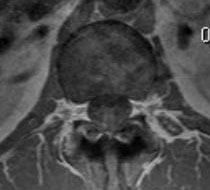
Fig. 5. A 28-year-old patient with intraspinal neurinoma at the level L3. The patient complained of lumboischialgia (back and leg pain).
A: The MRI shows the contrast enhancing tumour (arrows) that almost completely fills the spinal cord canal.
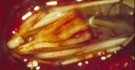
B: After the opening of the meninges one can see the tumour starting from the nerve roots.
C and D: Identification of the nerve root from which the tumour arises, above and below the tumour. This nerve root is without function.
E: Sectioning of the nerve root above and below the tumour.
F: Dissection of the tumour from the intact nerve roots.
G: Tumour removal in toto.
H: The postoperative MRI images show complete tumour removal. The patient is free of complaints. The neurological finding is normal.
Fig. 6. A 16-year-old girl with ependymoma of filum terminale at the level of L5. The patient complained of lumboischialgia (back and leg pain).
A: In the MRI one can see the large, contrast enhancing tumour that almost completely fills the spinal cord canal.
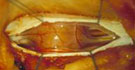
B: After the opening of the meninges one can see the tumour arising from the filum terminale (connective tissue strand without nervous function). Tumour removal after sectioning filum terminale above and below the tumour.
C: Spinal cord canal after tumour removal.
D: Tumour.
E: The postoperative MRI images show complete tumour removal. The patient is free of complaints. The neurological finding is normal.
Spinal cord tumours are rare (approx. 2% of all tumours of the central nerve system). The most common tumours are ependymomas (approx. 45%) and astrocytomas (approx. 35%). Haemangioblastomas constitute approx. 10%. Because these tumours are almost always benign, complete tumour removal is the aim of the surgery. Radiotherapy is not useful, because these tumours are not radiosensitive and the spinal cord is damaged in the case of a high dose of irradiation. The patients usually come to medical attention through pain. Later, sensory disturbances and insecure gate develop. The results of surgery on spinal cord tumours have become considerably better by the use of the microscopic dissection technique and intraoperative monitoring of the sensory and motor pathways. Ependymomas and haemangioblastomas can be isolated well from the spinal cord tissue and because of that well surgically removed. In the case of astrocytomas there is usually a diffuse growth with infiltration of the nerve pathways. Due to that in these tumours only partial tumour removal is possible. If untreated, these tumours almost always lead sooner or later to complete paraplegia.
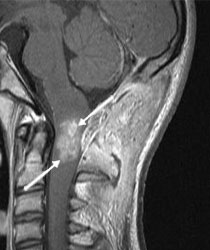
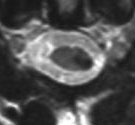
Fig. 7. A 58-year-old female patient with intramedullary ependymoma at the level of C 4-5. The patient complained of sensory disturbances in the left hand.
A: In the MRI the contrast enhancing tumour can be seen.
B: After the opening of the meninges the distended spinal cord can be seen.
C: The grey-red tumour has a clear border with the spinal cord and can be removed very well because of that.
D: The spinal cord after complete tumour removal.
E: In order to access the tumour, the vertebral arches from C 4, 5 and 6 had to be removed. After the tumour removal they are re-inserted and fixed with mini plates.
F and G: The X-ray images show the correct position of vertebral arches.
H: The female patient on the second day after the tumour removal without paralysis.
I: The MRI images 4 years after the surgery show complete tumour removal. The patient is free of complaints, except for fine motor disturbances of the left hand.
Fig. 8.
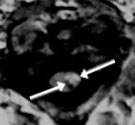
A: MRI of a 16-year-old boy with ependymoma of the upper cervical medulla (arrows). The boy presented with neck pain and vomiting. Despite the unfavourable position (danger of a high paraplegic syndrome with apnoea as well as arm and leg paralysis) surgery is the therapy of choice.
B: The arrows mark the remaining thin normal spinal cord tissue around the tumour (grey edge around the pale tumour).
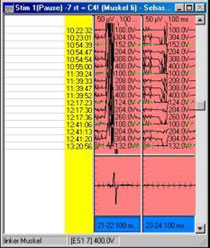
C: Monitoring of the motor-evoked potentials.
D and E: The follow-up MRI 3 months after the surgery shows complete tumour removal. The patient is neurologically normal except for minor clumsiness of the right hand.
Fig. 9.
A: MRI of a 34-year-old patient with cavernoma of the upper cervical medulla (arrows). The patient complained of paraesthesia in the left arm.
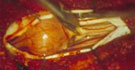
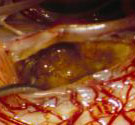
B: After the opening of the meninges a yellowish discoloration is visible at the lateral spinal cord at the level of the second cervical nerve roots.
C: Resection cave after cavernoma removal.
D: The follow-up MRI 2 years after the surgery shows complete tumour removal. However, the patient still complains of paraesthesia. Despite that, the cavernoma removal was useful because the haemorrhage danger with the risk of paraplegia was prevented.
Fig. 10.
A: MRI of a 50-year-old patient with a small haemangioblastoma of the medullar cone (lower end of the spinal cord) (arrow).
B: The medullar cone is cystically extended (arrows). The patient complained of urination disorders and ejaculation disorders.
C: The video shows the microsurgical tumour removal.
D: The follow-up MRI 3 months after the surgery shows complete tumour removal. The cyst is collapsed. The disorders resolved completely.
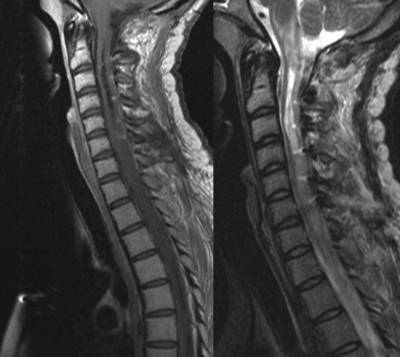
A 27-year-old female came presenting with neck pain and parasthesia in her both arms and hands, where MRI was performed showing intramedullary lesion that extend in the medulla just beyond the foramen magnum to the level of C5-6 disc.
Tumor was totally excised using irrigation-dissection microscopic technique with favorable outcome. Post-operative MRI showed no residual tumor.
|